

RACE to protect brains
- PMID: 20615310
- PMCID: PMC3229370
- DOI: 10.1308/003588410X12699663904916
RACE to protect brains
Abstract
Introduction: Rapid-access carotid endarterectomy (RACE) is an evidence-based treatment for symptomatic carotid stenosis. Our vascular centre aims to provide this service within 48 h of symptoms in appropriate patients. This study audits safety and efficacy of the first year of RACE.
Subjects and methods: A clear trust protocol was publicised for the RACE pathway. A prospective database was established for all carotid endarterectomies (CEAs) performed. Outcomes were compared between elective (ECE) and rapid-access operations.
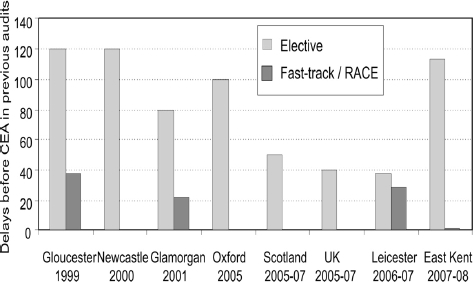
Results: In 1 year, 96 patients received CE; 20 were performed urgently. There were no significant differences in age or gender between ECE and RACE groups. Twenty-three (30%) of ECE were for asymptomatic stenoses; no other significant differences in surgical indication were seen. Of symptomatic ECE, 43% were for completed stroke versus 55% for RACE. Median delay between diagnosis and surgery was 113 days for elective and 2 days for RACE patients. There was one death following ECE (1.3%) and one stroke after RACE (5%), all not significant. Anaesthetic method did not influence outcome. The main reasons for delaying surgery in RACE patients were optimisation of patient fitness and availability of theatre time.
Conclusions: The RACE pathway dramatically reduces delay without compromising patient safety. In the first year of service, we have treated 50% of suitable patients within 48 h. Further education of patients and colleagues should reduce delay and improve outcomes for symptomatic carotid disease.
Figures
Similar articles
-
Endarterectomy for preventing stroke in symptomatic and asymptomatic carotid stenosis. Review of clinical trials and recommendations for surgical therapy.Heart Surg Forum. 1999;2(2):147-68. Heart Surg Forum. 1999. PMID: 11276473 Review.
-
Defining the threshold surgeon volume associated with improved patient outcomes for carotid endarterectomy.J Vasc Surg. 2020 Jul;72(1):209-218.e1. doi: 10.1016/j.jvs.2019.10.057. Epub 2020 Feb 19. J Vasc Surg. 2020. PMID: 32085960
-
Long-term stroke risk with carotid endarterectomy in patients with severe carotid stenosis.J Vasc Surg. 2021 Mar;73(3):983-991. doi: 10.1016/j.jvs.2020.06.124. Epub 2020 Jul 21. J Vasc Surg. 2021. PMID: 32707387
-
Outcomes for carotid endarterectomy in nonagenarians.J Vasc Surg. 2020 Jan;71(1):96-103. doi: 10.1016/j.jvs.2019.07.083. Epub 2019 Oct 11. J Vasc Surg. 2020. PMID: 31611107
-
[Surgical interventions also in primary prevention of stroke caused by significant carotid artery stenosis].Lakartidningen. 2004 May 13;101(20):1821-2, 1825-7. Lakartidningen. 2004. PMID: 15190770 Review. Swedish.
Cited by
-
Haematomas after carotid endarterectomy can be reduced by direct pressure to the neck postoperatively.Ann R Coll Surg Engl. 2018 Sep;100(7):580-583. doi: 10.1308/rcsann.2018.0109. Epub 2018 Jun 18. Ann R Coll Surg Engl. 2018. PMID: 29909667 Free PMC article.
References
-
- Rothwell PM, Buchan A, Johnston SC. Recent advances in management of transient ischaemic attacks and minor ischaemic strokes. Lancet Neurol. 2006;5:323–31. - PubMed
-
- Barnett HJ, Taylor DW, Eliasziw M, Fox AJ, Ferguson GG, et al. Benefit of carotid endarterectomy in patients with symptomatic moderate or severe stenosis. North American Symptomatic Carotid Endarterectomy Trial Collaborators. N Engl J Med. 1998;339:1415–25. - PubMed
-
- MRC European Carotid Surgery Trial (ECST) Randomised trial of endarterectomy for recently symptomatic carotid stenosis: final results of the MRC European Carotid Surgery Trial (ECST) Lancet. 1998;351:1379–87. - PubMed
-
- Naylor AR. Time is brain! Surgeon. 2007;5:23–30. - PubMed
-
- The Royal College of Physicians and Vascular Surgical Society. Great Britain and Ireland carotid endarterectomy audit. 2008. < http://www.vascularsociety.org.uk/Docs/GENERIC%20TRUST%20REPORT%20UK%20C...>.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources