

Central nervous system lymphoma: characteristic findings on traditional and advanced imaging
- PMID: 20616176
- PMCID: PMC8013157
- DOI: 10.3174/ajnr.A2171
Central nervous system lymphoma: characteristic findings on traditional and advanced imaging
Abstract
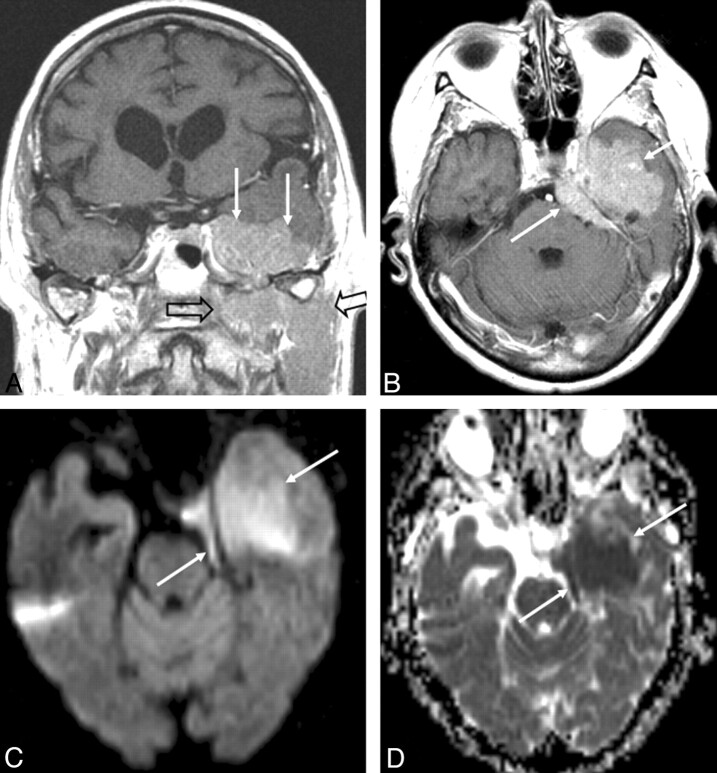
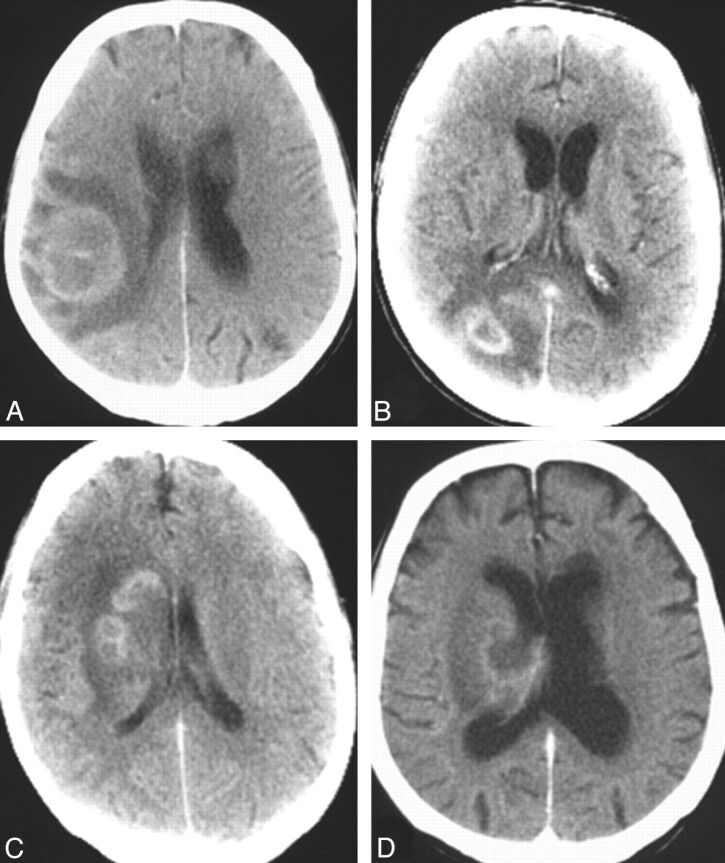
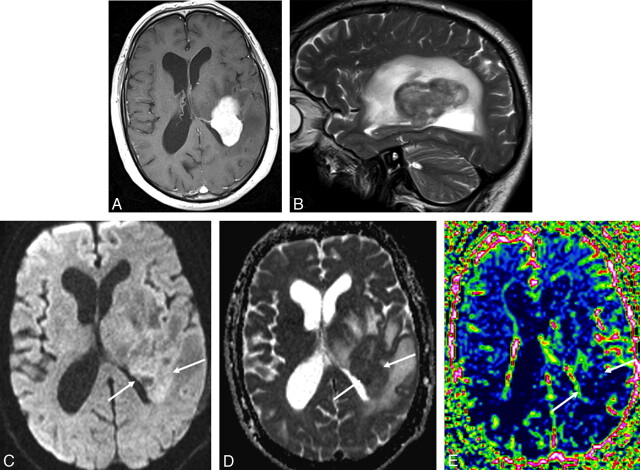
CNS lymphoma consists of 2 major subtypes: secondary CNS involvement by systemic lymphoma and PCNSL. Contrast-enhanced MR imaging is the method of choice for detecting CNS lymphoma. In leptomeningeal CNS lymphoma, representing two-thirds of secondary CNS lymphomas, imaging typically shows leptomeningeal, subependymal, dural, or cranial nerve enhancement. Single or multiple periventricular and/or superficial contrast-enhancing lesions are characteristic of parenchymal CNS lymphoma, representing one-third of secondary CNS lymphomas and almost 100% of PCNSLs. New CT and MR imaging techniques and metabolic imaging have demonstrated characteristic findings in CNS lymphoma, aiding in its differentiation from other CNS lesions. Advanced imaging techniques may, in the future, substantially improve the diagnostic accuracy of imaging, ultimately facilitating a noninvasive method of diagnosis. Furthermore, these imaging techniques may play a pivotal role in planning targeted therapies, prognostication, and monitoring treatment response.
Figures




References
-
- Wong ET. Management of central nervous system lymphomas using monoclonal antibodies: challenges and opportunities. Clin Cancer Res 2005; 11: 7151s– 57s - PubMed
-
- Mohile NA, Abrey LE. Primary central nervous system lymphoma. Semin Radiat Oncol 2007; 17: 223– 29 - PubMed
-
- Hill QA, Owen RG. CNS prophylaxis in lymphoma: who to target and what therapy to use. Blood Rev 2006; 20: 319– 32 - PubMed
-
- Montoto S, Lister TA. Secondary central nervous system lymphoma: risk factors and prophylaxis. Hematol Oncol Clin North Am 2005; 19: 751– 63 - PubMed
-
- Haldorsen IS, Krossnes BK, Aarseth JH, et al. . Increasing incidence and continued dismal outcome of primary central nervous system lymphoma in Norway 1989–2003: time trends in a 15-year national survey. Cancer 2007; 110: 1803– 14 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical