

Endovascular treatment of medically refractory cerebral vasospasm following aneurysmal subarachnoid hemorrhage
- PMID: 20616179
- PMCID: PMC4067264
- DOI: 10.3174/ajnr.A2183
Endovascular treatment of medically refractory cerebral vasospasm following aneurysmal subarachnoid hemorrhage
Abstract
Background and purpose: CV following aneurysmal SAH is a significant cause of morbidity and mortality. We review our experiences using PTA and IA verapamil infusion for treating medically refractory cases.
Materials and methods: We performed a retrospective review of patients with SAH admitted from July 2003 to January 2008.
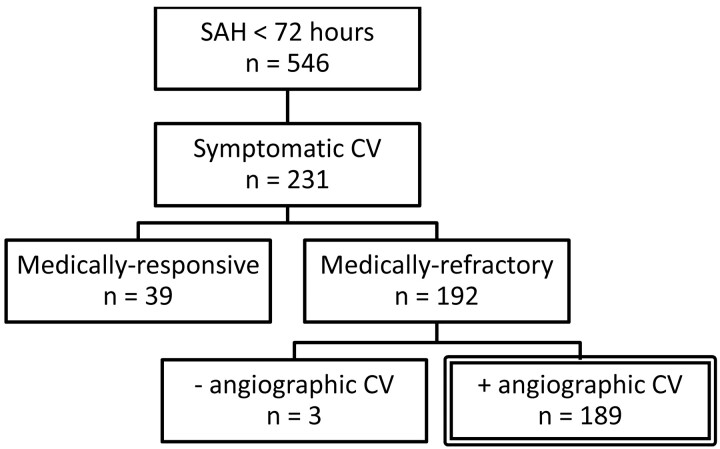
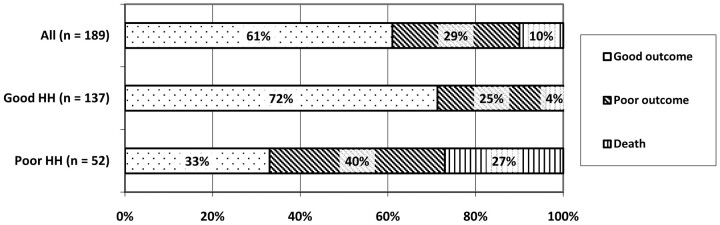
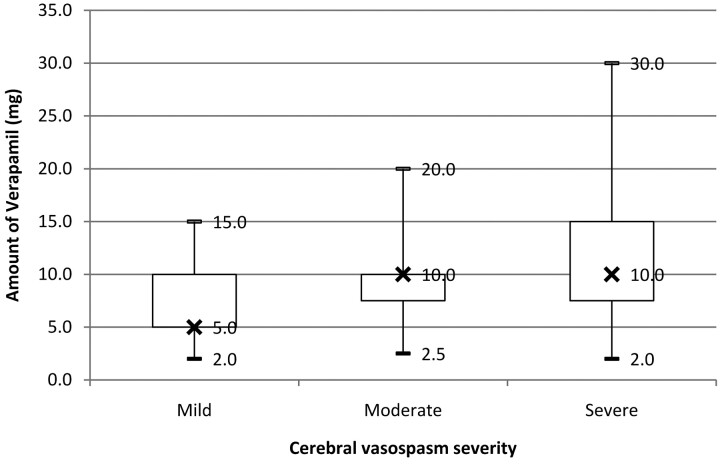
Results: Of 546 patients admitted within 72 hours of symptom onset, 231 patients (42%) developed symptomatic CV and 189 patients (35%) required endovascular therapy. A total of 346 endovascular sessions were performed consisting of 1 single angioplasty, 286 IA verapamil infusions, and 59 combined treatments. PTA was performed on 151 vessel segments, and IA verapamil was infused in 720 vessel segments. IA verapamil doses ranged from 2.0 to 30.0 mg per vessel segment and from 3.0 to 55.0 mg per treatment session. Repeat treatments were necessary in 102 patients (54%) for persistent, recurrent, or worsening CV. There were 6 treatment-related complications, of which 2 resulted in clinical worsening. No deaths were attributable to endovascular therapy. At follow-up, 115 patients (61%) had a good outcome and 55 patients (29%) had a poor outcome. Sixteen patients died from causes related to SAH, while 3 died from other medical complications.
Conclusions: Endovascular treatments are an integral part of managing patients with medically refractory CV. In our experience, PTA and IA verapamil are safe, with a low complication rate, but further studies are required to determine appropriate patient selection and treatment efficacy.
Figures
References
-
- Kassell NF, Torner JC, Haley EC, Jr, et al. . The International Cooperative Study on the Timing of Aneurysm Surgery. Part 1. Overall management results. J Neurosurg 1990;73:18–36 - PubMed
-
- Yundt KD, Grubb RL, Jr, Diringer MN, et al. . Autoregulatory vasodilation of parenchymal vessels is impaired during cerebral vasospasm. J Cereb Blood Flow Metab 1998;18:419–24 - PubMed
-
- Voldby B, Enevoldsen EM, Jensen FT. Regional CBF, intraventricular pressure, and cerebral metabolism in patients with ruptured intracranial aneurysms. J Neurosurg 1985;62:48–58 - PubMed
-
- Ohkuma H, Manabe H, Tanaka M, et al. . Impact of cerebral microcirculatory changes on cerebral blood flow during cerebral vasospasm after aneurysmal subarachnoid hemorrhage. Stroke 2000;31:1621–27 - PubMed
-
- Ishii R. Regional cerebral blood flow in patients with ruptured intracranial aneurysms. J Neurosurg 1979;50:587–94 - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical