

The importance of adjusting for potential confounders in Bayesian hierarchical models synthesising evidence from randomised and non-randomised studies: an application comparing treatments for abdominal aortic aneurysms
- PMID: 20618973
- PMCID: PMC2916004
- DOI: 10.1186/1471-2288-10-64
The importance of adjusting for potential confounders in Bayesian hierarchical models synthesising evidence from randomised and non-randomised studies: an application comparing treatments for abdominal aortic aneurysms
Abstract
Background: Informing health care decision making may necessitate the synthesis of evidence from different study designs (e.g., randomised controlled trials, non-randomised/observational studies). Methods for synthesising different types of studies have been proposed, but their routine use requires development of approaches to adjust for potential biases, especially among non-randomised studies. The objective of this study was to extend a published Bayesian hierarchical model to adjust for bias due to confounding in synthesising evidence from studies with different designs.
Methods: In this new methodological approach, study estimates were adjusted for potential confounders using differences in patient characteristics (e.g., age) between study arms. The new model was applied to synthesise evidence from randomised and non-randomised studies from a published review comparing treatments for abdominal aortic aneurysms. We compared the results of the Bayesian hierarchical model adjusted for differences in study arms with: 1) unadjusted results, 2) results adjusted using aggregate study values and 3) two methods for downweighting the potentially biased non-randomised studies. Sensitivity of the results to alternative prior distributions and the inclusion of additional covariates were also assessed.
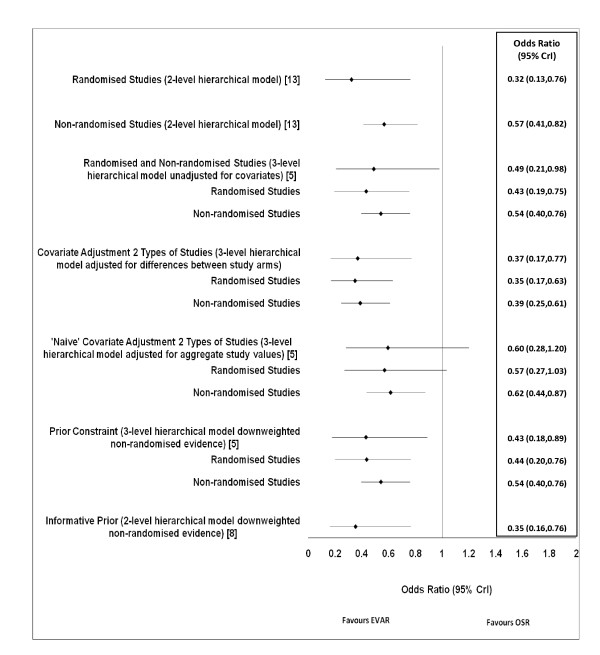
Results: In the base case analysis, the estimated odds ratio was 0.32 (0.13,0.76) for the randomised studies alone and 0.57 (0.41,0.82) for the non-randomised studies alone. The unadjusted result for the two types combined was 0.49 (0.21,0.98). Adjusted for differences between study arms, the estimated odds ratio was 0.37 (0.17,0.77), representing a shift towards the estimate for the randomised studies alone. Adjustment for aggregate values resulted in an estimate of 0.60 (0.28,1.20). The two methods used for downweighting gave odd ratios of 0.43 (0.18,0.89) and 0.35 (0.16,0.76), respectively. Point estimates were robust but credible intervals were wider when using vaguer priors.
Conclusions: Covariate adjustment using aggregate study values does not account for covariate imbalances between treatment arms and downweighting may not eliminate bias. Adjustment using differences in patient characteristics between arms provides a systematic way of adjusting for bias due to confounding. Within the context of a Bayesian hierarchical model, such an approach could facilitate the use of all available evidence to inform health policy decisions.
Figures
References
-
- International Network of Agencies for Health Technology Assessment. http://www.inahta.org/HTA
-
- Centre for Reviews and Dissemination. Systematic Reviews: CRD's guidance undertaking reviews in health care. York: University of York; 2009.
-
- Gordis L. Epidemiology. Philadelphia: Elsevier Inc; 2004.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
