

Intra-myocardial biomaterial injection therapy in the treatment of heart failure: Materials, outcomes and challenges
- PMID: 20619368
- PMCID: PMC3208237
- DOI: 10.1016/j.actbio.2010.06.039
Intra-myocardial biomaterial injection therapy in the treatment of heart failure: Materials, outcomes and challenges
Abstract
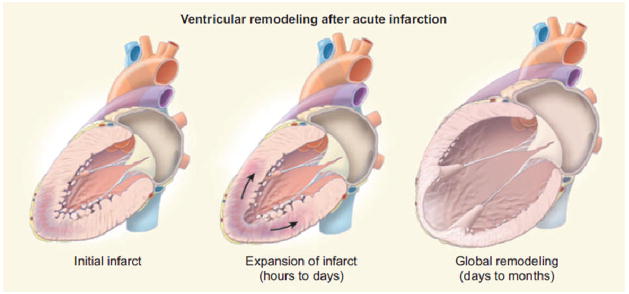
Heart failure initiated by coronary artery disease and myocardial infarction (MI) is a widespread, debilitating condition for which there are a limited number of options to prevent disease progression. Intra-myocardial biomaterial injection following MI theoretically provides a means to reduce the stresses experienced by the infarcted ventricular wall, which may alter the pathological remodeling process in a positive manner. Furthermore, biomaterial injection provides an opportunity to concurrently introduce cellular components and depots of bioactive agents. Biologically derived, synthetic and hybrid materials have been applied, as well as materials designed expressly for this purpose, although optimal design parameters, including degradation rate and profile, injectability, elastic modulus and various possible bioactivities, largely remain to be elucidated. This review seeks to summarize the current body of growing literature where biomaterial injection, with and without concurrent pharmaceutical or cellular delivery, has been pursued to improve functional outcomes following MI. The literature to date generally demonstrates acute functional benefits associated with biomaterial injection therapy across a broad variety of animal models and material compositions. Further functional improvements have been reported when cellular or pharmaceutical agents have been incorporated into the delivery system. Despite these encouraging early results, the specific mechanisms behind the observed functional improvements remain to be fully explored and future studies employing hypothesis-driven material design and selection may increase the potential of this approach to alleviate the morbidity and mortality of heart failure.
Copyright © 2010 Acta Materialia Inc. Published by Elsevier Ltd. All rights reserved.
Figures
References
-
- Jessup M, Brozena S. Heart failure. N Engl J Med. 2003;348:2007–18. - PubMed
-
- Hannan EL, et al. A comparison of three-year survival after coronary artery bypass graft surgery and percutaneous transluminal coronary angioplasty. J Am Coll Cardiol. 1999;33:63–72. - PubMed
-
- Hannan EL, et al. Long-term outcomes of coronary-artery bypass grafting versus stent implantation. N Engl J Med. 2005;352:2174–83. - PubMed
-
- Nelson GS, et al. Left ventricular or biventricular pacing improves cardiac function at diminished energy cost in patients with dilated cardiomyopathy and left bundle-branch block. Circulation. 2000;102:3053–9. - PubMed
-
- Flather MD, et al. Long-term ACE-inhibitor therapy in patients with heart failure or left-ventricular dysfunction: a systematic overview of data from individual patients. ACE-Inhibitor Myocardial Infarction Collaborative Group. Lancet. 2000;355:1575–81. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
