

Prolonged infectiousness of tuberculosis patients in a directly observed therapy short-course program with standardized therapy
- PMID: 20624064
- PMCID: PMC4465448
- DOI: 10.1086/655127
Prolonged infectiousness of tuberculosis patients in a directly observed therapy short-course program with standardized therapy
Abstract
Background: Effective tuberculosis control is compromised by a lack of clarity about the timeframe of viable Mycobacterium tuberculosis shedding after treatment initiation under programmatic conditions. This study quantifies time to conversion from smear and culture positivity to negativity in unselected tuberculosis patients receiving standardized therapy in a directly observed therapy short-course (DOTS) program.
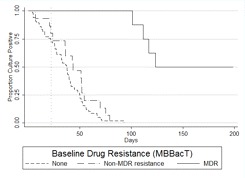
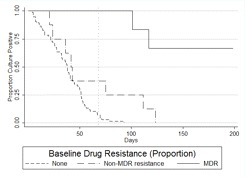
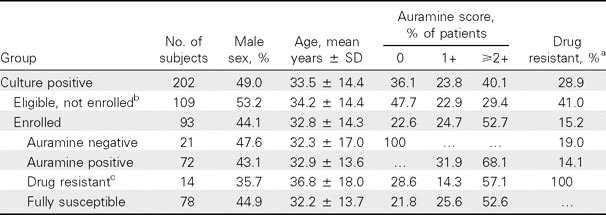
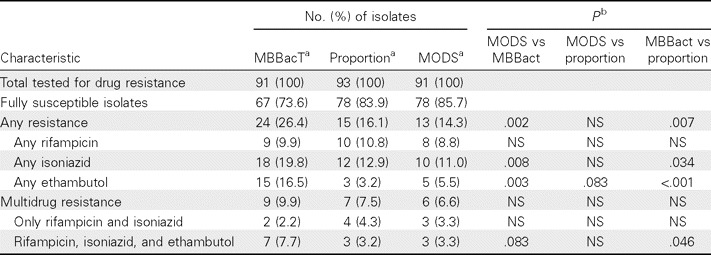
Methods: Longitudinal cohort study following up 93 adults initiating tuberculosis therapy in Lima, Peru. Baseline culture and drug susceptibility tests (DSTs) were performed using the MBBacT, proportion, and microscopic observation drug susceptibility (MODS) methods. Smear microscopy and MODS liquid culture were performed at baseline and weekly for 4 weeks then every other week for 26 weeks.
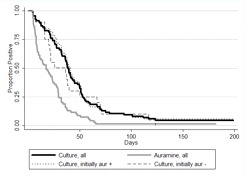
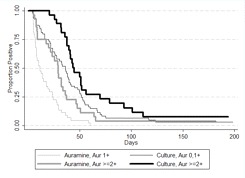
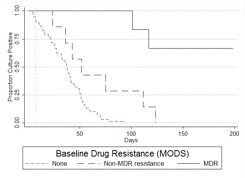
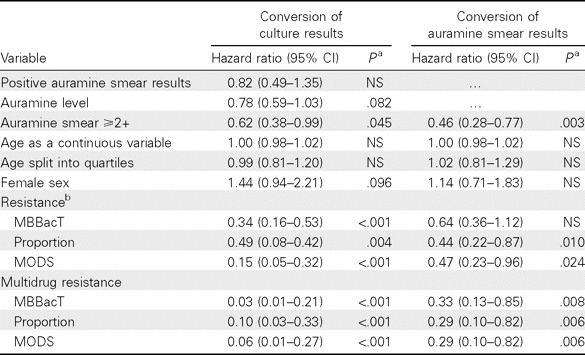
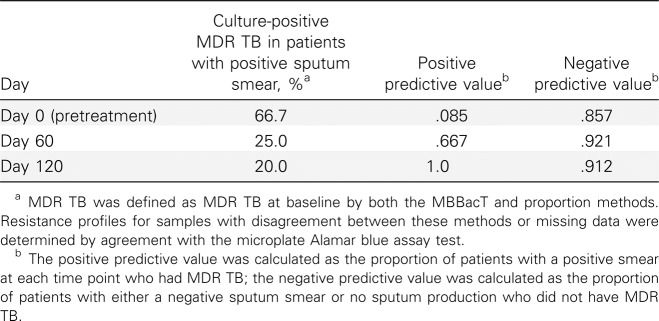
Results: Median conversion time from culture positivity to culture negativity of 38.5 days was unaffected by baseline smear status. Patients with fully susceptible tuberculosis had a median time to culture conversion of 37 days; 10% remained culture positive at day 60. Delayed culture conversion was associated with multidrug resistance, regardless of DST method used; non-multidrug resistance as defined by the proportion method and MODS (but not MBBacT) was also associated with delay. Persistent day 60 smear positivity yielded positive and negative predictive values of 67% and 92%, respectively, for detecting multidrug resistance.
Conclusions: Smear and culture conversion in treated tuberculosis patients takes longer than is conventionally believed, even with fully susceptible disease, and must be accounted for in tuberculosis treatment and prevention programs. Persistent day 60 smear positivity is a poor predictor of multidrug resistance. The industrialized-world convention of universal baseline DST for tuberculosis patients should become the standard of care in multidrug resistance-affected resource-limited settings.
Figures
Comment in
-
Does my patient have multidrug-resistant tuberculosis?Clin Infect Dis. 2010 Aug 15;51(4):379-80. doi: 10.1086/655128. Clin Infect Dis. 2010. PMID: 20624063 No abstract available.
-
Serial acid fast bacilli smear and culture conversion rates over 26 weeks in a cohort of 93 sputum culture–positive tuberculosis (TB).Clin Infect Dis. 2011 Feb 15;52(4):554-6. doi: 10.1093/cid/ciq182. Clin Infect Dis. 2011. PMID: 21258108 Free PMC article. No abstract available.
References
-
- World Health Organization. Report WHO/HTM/TB/ 2008.393. Geneva, Switzerland: World Health Organization; 2008. Global tuberculosis control: surveillance, planning, financing: WHO report 2008.
-
- Stop TB Partnership World Health Organization. Report WHO/HTM/STB/2006.35. Geneva, Switzerland: World Health Organization; 2006. Global plan to stop TB 2006–2015.
-
- The effect of tuberculosis control in China. Lancet. 2004;364:417–422. - PubMed
-
- Suarez PG, Watt CJ, Alarcon E, et al. The dynamics of tuberculosis in response to 10 years of intensive control effort in Peru. J Infect Dis. 2001;184:473–478. - PubMed
-
- Huong NT, Duong BD, Co NV, et al. Tuberculosis epidemiology in six provinces of Vietnam after the introduction of the DOTS strategy. Int J Tuberc Lung Dis. 2006;10:963–969. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
