

Midazolam versus diazepam for the treatment of status epilepticus in children and young adults: a meta-analysis
- PMID: 20624136
- PMCID: PMC4149412
- DOI: 10.1111/j.1553-2712.2010.00751.x
Midazolam versus diazepam for the treatment of status epilepticus in children and young adults: a meta-analysis
Abstract
Background: Rapid treatment of status epilepticus (SE) is associated with better outcomes. Diazepam and midazolam are commonly used, but the optimal agent and administration route is unclear.
Objectives: The objective was to determine by systematic review if nonintravenous (non-IV) midazolam is as effective as diazepam, by any route, in terminating SE seizures in children and adults. Time to seizure cessation and respiratory complications was examined.
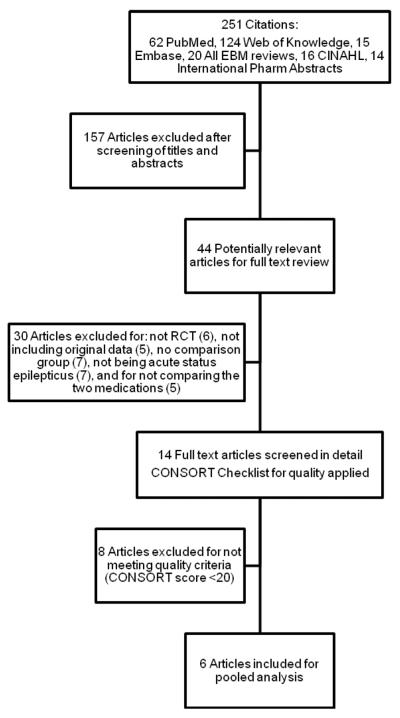
Methods: We performed a search of PubMed, Web of Knowledge, Embase, Cochrane Database of Systematic Reviews, Database of Abstracts of Reviews of Effects, American College of Physicians Journal Club, Cochrane Central Register of Controlled Trials, the Cumulative Index to Nursing and Allied Health Literature, and International Pharmaceutical Abstracts for studies published January 1, 1950, through July 4, 2009. English language quasi-experimental or randomized controlled trials comparing midazolam and diazepam as first-line treatment for SE, and meeting the Consolidated Standards of Reporting Trials (CONSORT)-based quality measures, were eligible. Two reviewers independently screened studies for inclusion and extracted outcomes data. Administration routes were stratified as non-IV (buccal, intranasal, intramuscular, rectal) or IV. Fixed-effects models generated pooled statistics.
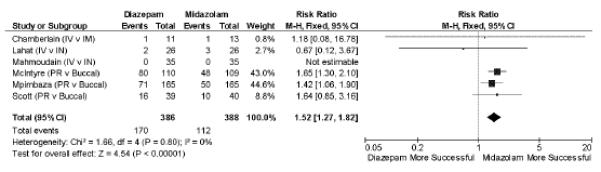
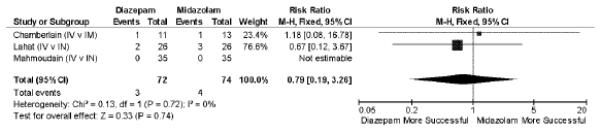
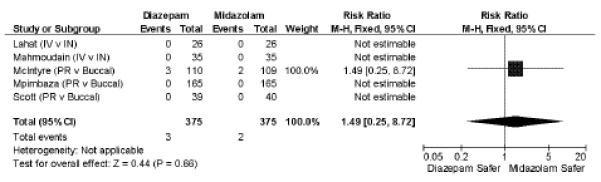
Results: Six studies with 774 subjects were included. For seizure cessation, midazolam, by any route, was superior to diazepam, by any route (relative risk [RR] = 1.52; 95% confidence interval [CI] = 1.27 to 1.82). Non-IV midazolam is as effective as IV diazepam (RR = 0.79; 95% CI = 0.19 to 3.36), and buccal midazolam is superior to rectal diazepam in achieving seizure control (RR = 1.54; 95% CI = 1.29 to 1.85). Midazolam was administered faster than diazepam (mean difference = 2.46 minutes; 95% CI = 1.52 to 3.39 minutes) and had similar times between drug administration and seizure cessation. Respiratory complications requiring intervention were similar, regardless of administration route (RR = 1.49; 95% CI = 0.25 to 8.72).
Conclusions: Non-IV midazolam, compared to non-IV or IV diazepam, is safe and effective in treating SE. Comparison to lorazepam, evaluation in adults, and prospective confirmation of safety and efficacy is needed.
(c) 2010 by the Society for Academic Emergency Medicine.
Figures
References
-
- Huff JS, Morris DL, Kothari RU, Gibbs MA. Emergency department management of patients with seizures: a multicenter study. Acad Emerg Med. 2001;8:622–8. - PubMed
-
- Epilepsy Foundation [Accessed Feb 28, 2010];Epilepsy and seizure statistics. Available at: http://www.epilepsyfoundation.org/about/statistics.cfm.
-
- Shinnar S, Berg AT, Moshe SL, Shinnar R. How long do new-onset seizures in children last? Ann Neurol. 2001;49(5):659–64. - PubMed
-
- Theodore WH, Porter RJ, Albert P, et al. The secondarily generalized tonic-clonic seizure: a videotape analysis. Neurology. 1994;44(8):1403–7. - PubMed
-
- DeLorenzo RJ, Hauser WA, Towne AR, et al. A prospective, population-based epidemiologic study of status epilepticus in Richmond, Virginia. Neurology. 1996;46(4):1029–35. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
