

Degenerative mitral valve regurgitation: best practice revolution
- PMID: 20624767
- PMCID: PMC2921508
- DOI: 10.1093/eurheartj/ehq222
Degenerative mitral valve regurgitation: best practice revolution
Abstract
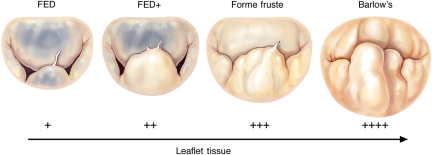
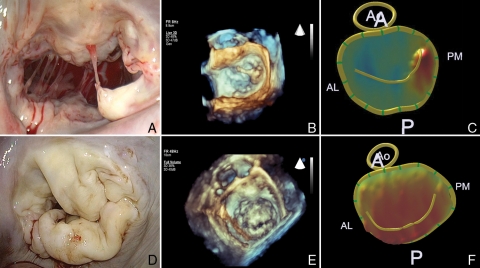
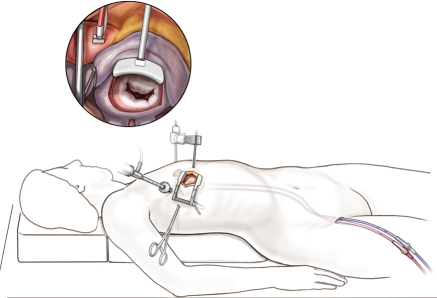
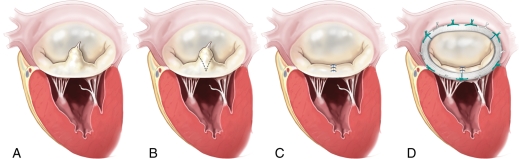
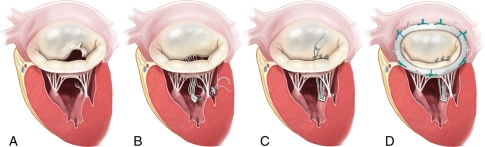
Degenerative mitral valve disease often leads to leaflet prolapse due to chordal elongation or rupture, and resulting in mitral valve regurgitation. Guideline referral for surgical intervention centres primarily on symptoms and ventricular dysfunction. The recommended treatment for degenerative mitral valve disease is mitral valve reconstruction, as opposed to valve replacement with a bioprosthetic or mechanical valve, because valve repair is associated with improved event free survival. Recent studies have documented a significant number of patients are not referred in a timely fashion according to established guidelines, and when they are subjected to surgery, an alarming number of patients continue to undergo mitral valve replacement. The debate around appropriate timing of intervention for asymptomatic severe mitral valve regurgitation has put additional emphasis on targeted surgeon referral and the need to ensure a very high rate of mitral valve repair, particularly in the non-elderly population. Current clinical practice remains suboptimal for many patients, and this review explores the need for a 'best practice revolution' in the field of degenerative mitral valve regurgitation.
Figures
References
-
- Enriquez-Sarano M, Akins CW, Vahanian A. Mitral regurgitation. Lancet. 2009;373:1382–1394. doi:10.1016/S0140-6736(09)60692-9. - DOI - PubMed
-
- Anders S, Said S, Schulz F, Puschel K. Mitral valve prolapse syndrome as cause of sudden death in young adults. Forensic Sci Int. 2007;171:127–130. doi:10.1016/j.forsciint.2006.10.011. - DOI - PubMed
-
- Carabello BA. The current therapy for mitral regurgitation. J Am Coll Cardiol. 2008;52:319–326. doi:10.1016/j.jacc.2008.02.084. - DOI - PubMed
-
- Enriquez-Sarano M, Avierinos JF, Messika-Zeitoun D, Detaint D, Capps M, Nkomo V, Scott C, Schaff HV, Tajik AJ. Quantitative determinants of the outcome of asymptomatic mitral regurgitation. N Engl J Med. 2005;352:875–883. doi:10.1056/NEJMoa041451. - DOI - PubMed
-
- Kang DH, Kim JH, Rim JH, Kim MJ, Yun SC, Song JM, Song H, Choi KJ, Song JK, Lee JW. Comparison of early surgery versus conventional treatment in asymptomatic severe mitral regurgitation. Circulation. 2009;119:797–804. doi:10.1161/CIRCULATIONAHA.108.802314. - DOI - PubMed
