

Intracranial pressure-monitoring systems in children with traumatic brain injury: combining therapeutic and diagnostic tools
- PMID: 20625341
- PMCID: PMC3670608
- DOI: 10.1097/PCC.0b013e3181e8b3ee
Intracranial pressure-monitoring systems in children with traumatic brain injury: combining therapeutic and diagnostic tools
Abstract
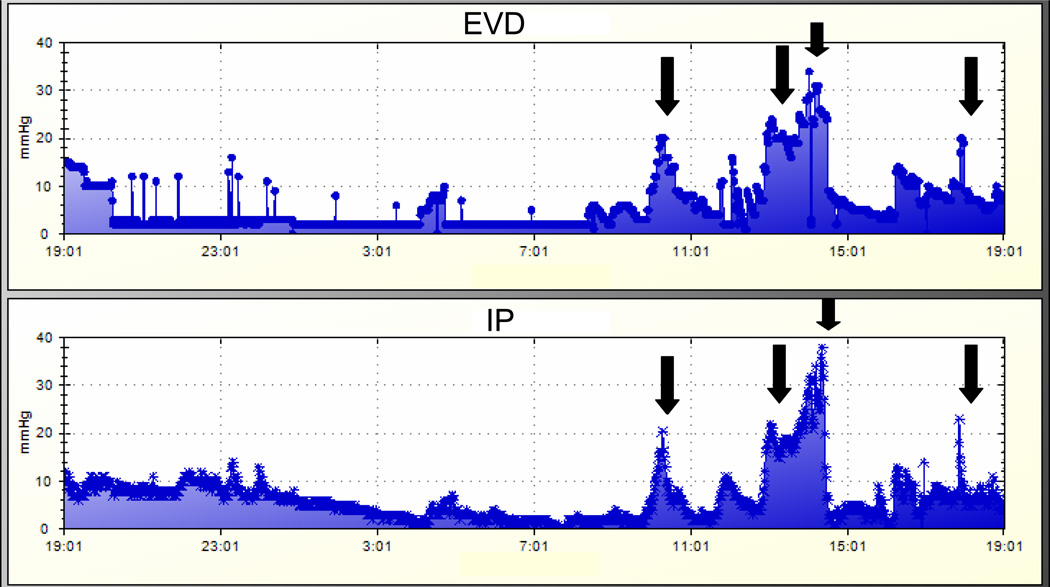
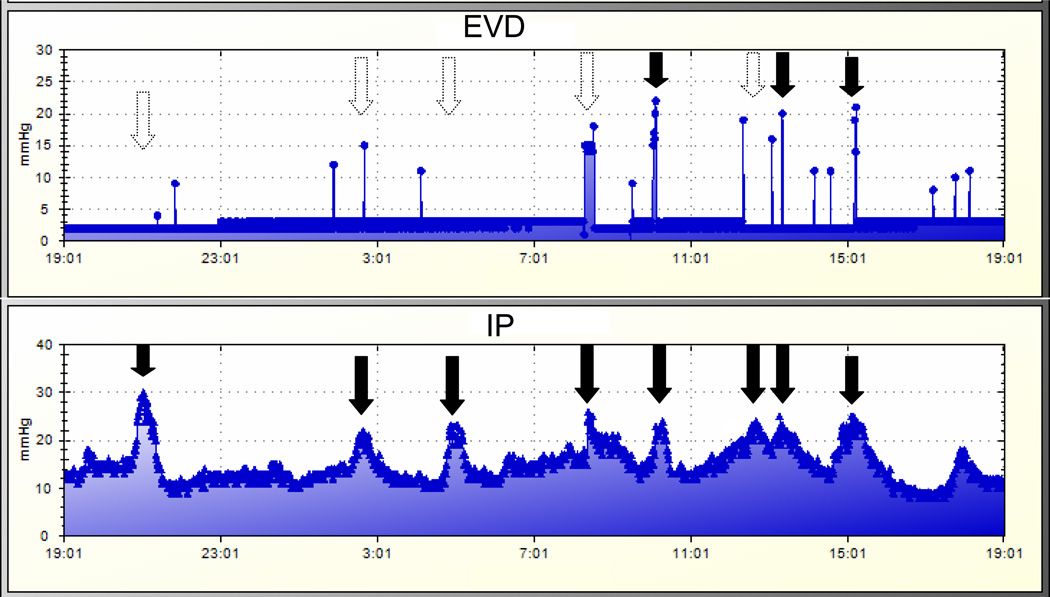
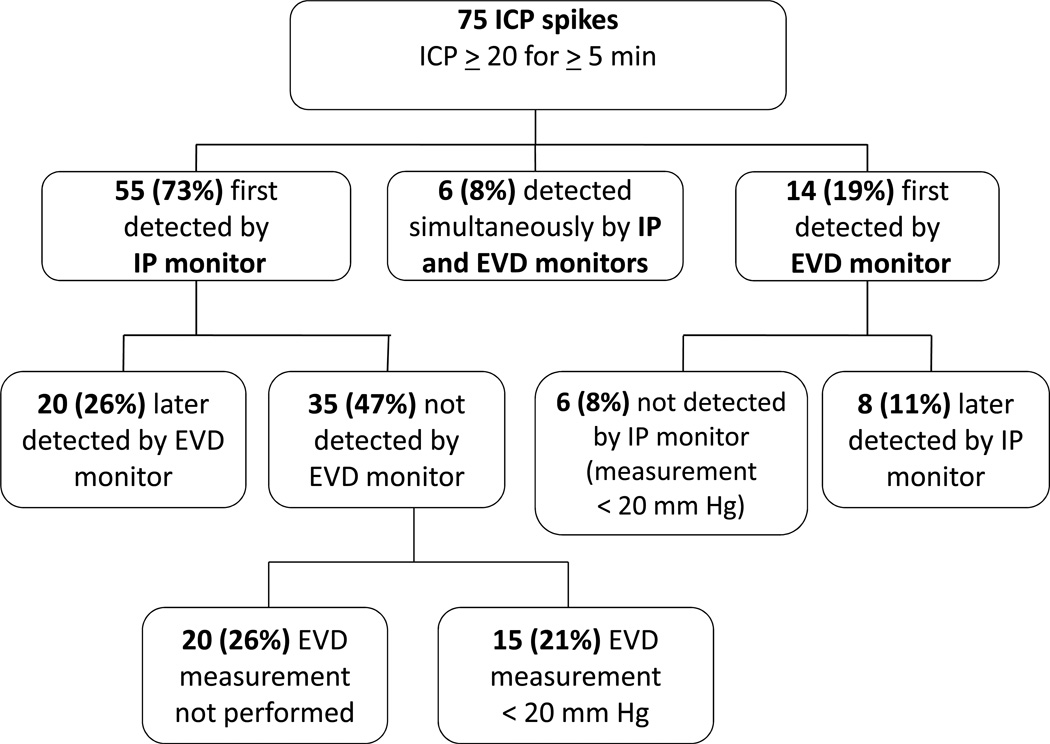
Objective: To compare the correlation of intracranial pressure (ICP) measurement and time to detection of ICP crises (defined as ICP ≥ 20 mm Hg for ≥ 5 mins) between an intraparenchymal (IP) monitor and external ventricular drain (EVD) in children for whom continuous cerebrospinal fluid diversion was used as a therapy for severe traumatic brain injury.
Setting: Academic, pediatric intensive care unit.
Design: Retrospective review of a prospectively collected pediatric neurotrauma database.
Patients: Children with severe traumatic brain injury (Glasgow Coma Scale score of ≤ 8) who underwent ICP monitoring with both IP and EVD techniques were studied. In cohort 1 (n = 58), hourly ICP measurements were extracted from the medical record; in cohort 2 (n = 4), ICP measurements were collected every minute by an automated data-collection system.
Measurements and main results: The mean absolute difference in ICP (|N5ICP|N5) and intraclass correlation coefficients were calculated. Timing to detection of ICP crises was analyzed. Data were expressed as mean ± sem. For cohort 1, 7,387 hrs of data were analyzed; 399 hrs (23,940 mins) were analyzed for cohort 2. In cohort 1, the |N5ICP|N5 was 3.10 ± 0.04 mm Hg (intraclass correlation coefficients = 0.98, p < .001). The |N5ICP|N5 in cohort 2 was 3.30 ± 0.05 mm Hg (intraclass correlation coefficients = 0.98, p < .001). In cohort 2, a total of 75 ICP crises were observed. Fifty-five (73%) were detected first by the IP monitor, of which 35 were not identified by the EVD monitor. Time between IP and EVD detection of a crisis was 12.60 ± 2.34 mins.
Conclusion: EVD and IP measurements of ICP were highly correlated, although intermittent EVD ICP measurements may fail to identify ICP events when continuously draining cerebrospinal fluid. In institutions that use continuous cerebrospinal fluid diversion as a therapy, a two-monitor system may be valuable for accomplishing monitoring and therapeutic goals.
Figures
Comment in
-
Intracranial pressure monitoring in children: back to basics.Pediatr Crit Care Med. 2011 Sep;12(5):600-1. doi: 10.1097/PCC.0b013e3182257a5e. Pediatr Crit Care Med. 2011. PMID: 21897164 No abstract available.
References
-
- Adelson PD, Bratton SL, et al. Guidelines for the acute medical management of severe traumatic brain injury in infants, children, and adolescents. Pediatr Crit Care Med. 2003;4(3) Suppl:S1–S75. - PubMed
-
- Ostrup RC, Luerssen TG, Marshall LF, Zornow MH. Continuous monitoring of intracranial pressure with a miniaturized fiberoptic device. J Neurosurg. 1987;67(2):206–209. - PubMed
-
- Gambardella G, Zaccone C, Cardia E, Tomasello F. Intracranial pressure monitoring in children: comparison of external ventricular device with the fiberoptic system. Childs Nerv Syst. 1993;9(8):470–473. - PubMed
-
- Chambers KR, Kane PJ, Choksey MS, Mendelow AD. An evaluation of the camino ventricular bolt system in clinical practice. Neurosurgery. 1993;33(5):866–868. - PubMed
-
- Piek J, Bock WJ. Continuous monitoring of cerebral tissue pressure in neurosurgical practice--experiences with 100 patients. Intensive Care Med. 1990;16(3):184–188. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
