

Stable and unstable malaria hotspots in longitudinal cohort studies in Kenya
- PMID: 20625549
- PMCID: PMC2897769
- DOI: 10.1371/journal.pmed.1000304
Stable and unstable malaria hotspots in longitudinal cohort studies in Kenya
Erratum in
- PLoS Med. 2011 Feb;8(2). doi: 10.1371/annotation/592709c8-8f86-4f40-968b-1e7e051ab491 doi: 10.1371/annotation/592709c8-8f86-4f40-968b-1e7e051ab491
Abstract
Background: Infectious diseases often demonstrate heterogeneity of transmission among host populations. This heterogeneity reduces the efficacy of control strategies, but also implies that focusing control strategies on "hotspots" of transmission could be highly effective.
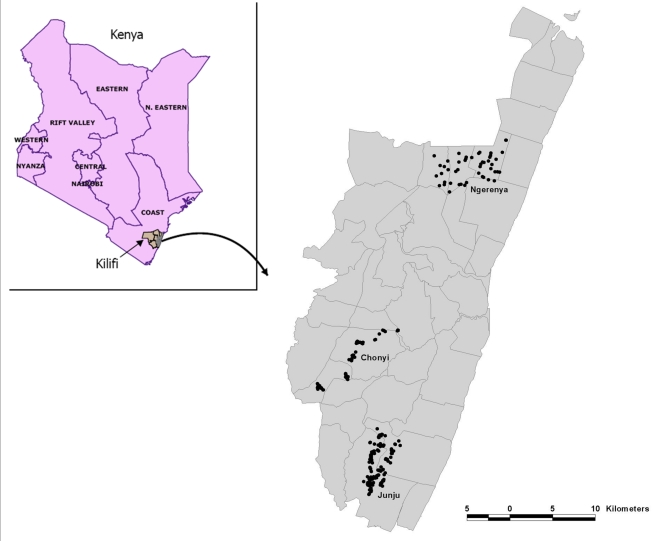
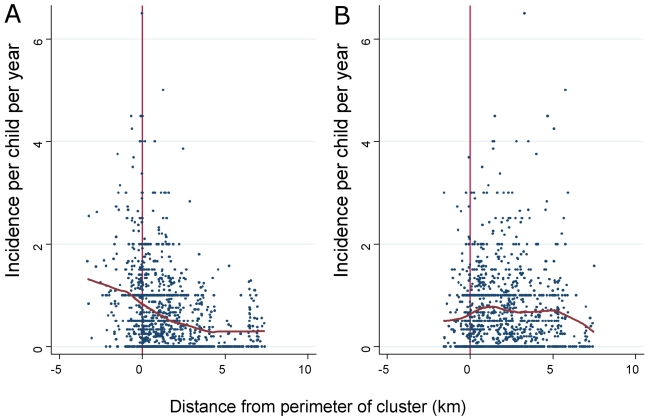
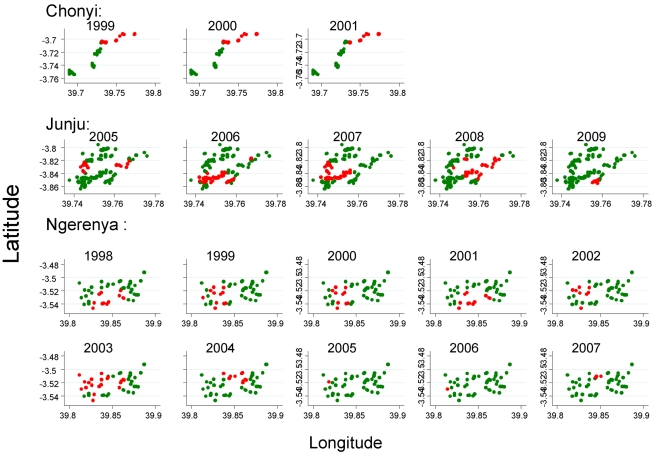
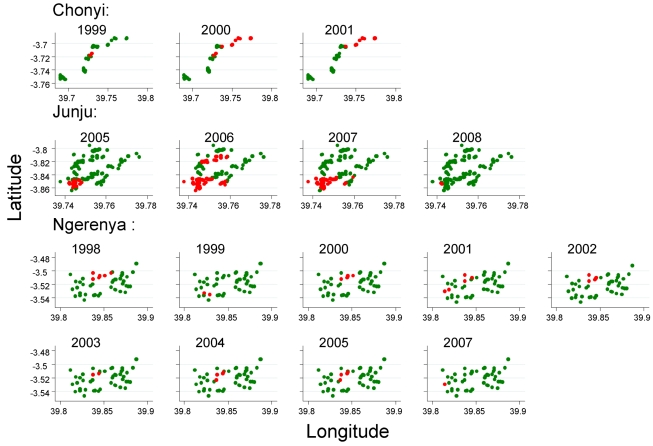
Methods and findings: In order to identify hotspots of malaria transmission, we analysed longitudinal data on febrile malaria episodes, asymptomatic parasitaemia, and antibody titres over 12 y from 256 homesteads in three study areas in Kilifi District on the Kenyan coast. We examined heterogeneity by homestead, and identified groups of homesteads that formed hotspots using a spatial scan statistic. Two types of statistically significant hotspots were detected; stable hotspots of asymptomatic parasitaemia and unstable hotspots of febrile malaria. The stable hotspots were associated with higher average AMA-1 antibody titres than the unstable clusters (optical density [OD] = 1.24, 95% confidence interval [CI] 1.02-1.47 versus OD = 1.1, 95% CI 0.88-1.33) and lower mean ages of febrile malaria episodes (5.8 y, 95% CI 5.6-6.0 versus 5.91 y, 95% CI 5.7-6.1). A falling gradient of febrile malaria incidence was identified in the penumbrae of both hotspots. Hotspots were associated with AMA-1 titres, but not seroconversion rates. In order to target control measures, homesteads at risk of febrile malaria could be predicted by identifying the 20% of homesteads that experienced an episode of febrile malaria during one month in the dry season. That 20% subsequently experienced 65% of all febrile malaria episodes during the following year. A definition based on remote sensing data was 81% sensitive and 63% specific for the stable hotspots of asymptomatic malaria.
Conclusions: Hotspots of asymptomatic parasitaemia are stable over time, but hotspots of febrile malaria are unstable. This finding may be because immunity offsets the high rate of febrile malaria that might otherwise result in stable hotspots, whereas unstable hotspots necessarily affect a population with less prior exposure to malaria.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Smith DL, McKenzie FE, Snow RW, Hay SI. Revisiting the basic reproductive number for malaria and its implications for malaria control. PLoS Biol. 2007;5:e42. doi: 10.1371/journal.pbio.0050042. - DOI - PMC - PubMed
-
- Gamage-Mendis AC, Carter R, Mendis C, De Zoysa AP, Herath PR, et al. Clustering of malaria infections within an endemic population: risk of malaria associated with the type of housing construction. Am J Trop Med Hyg. 1991;45:77–85. - PubMed
-
- Ghebreyesus TA, Haile M, Witten KH, Getachew A, Yohannes M, et al. Household risk factors for malaria among children in the Ethiopian highlands. Trans R Soc Trop Med Hyg. 2000;94:17–21. - PubMed
