

Plaque and deposits in nine human stone diseases
- PMID: 20625890
- PMCID: PMC3175811
- DOI: 10.1007/s00240-010-0296-z
Plaque and deposits in nine human stone diseases
Abstract
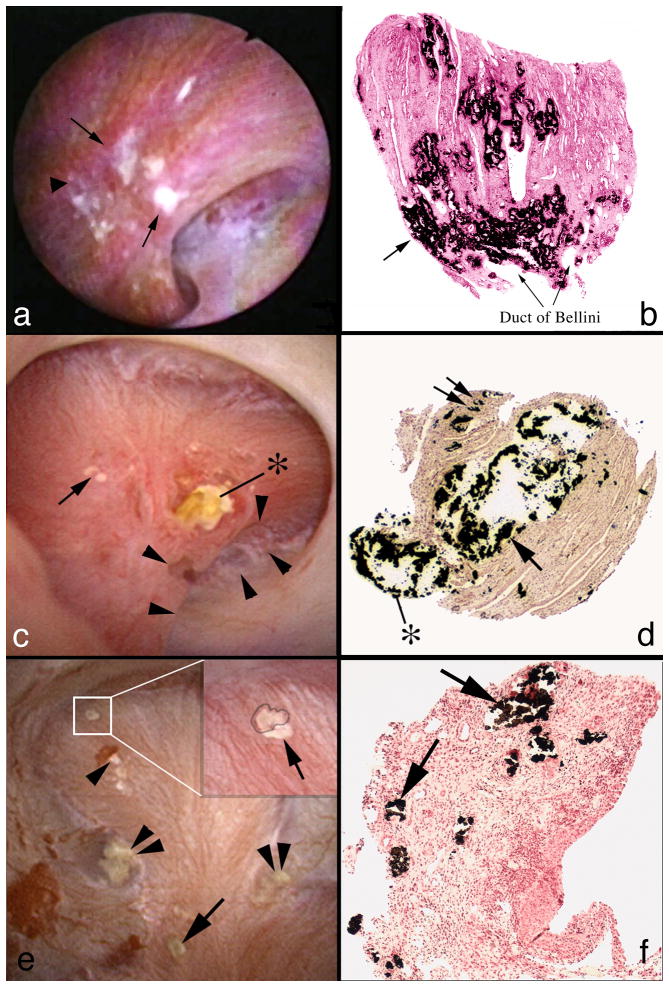
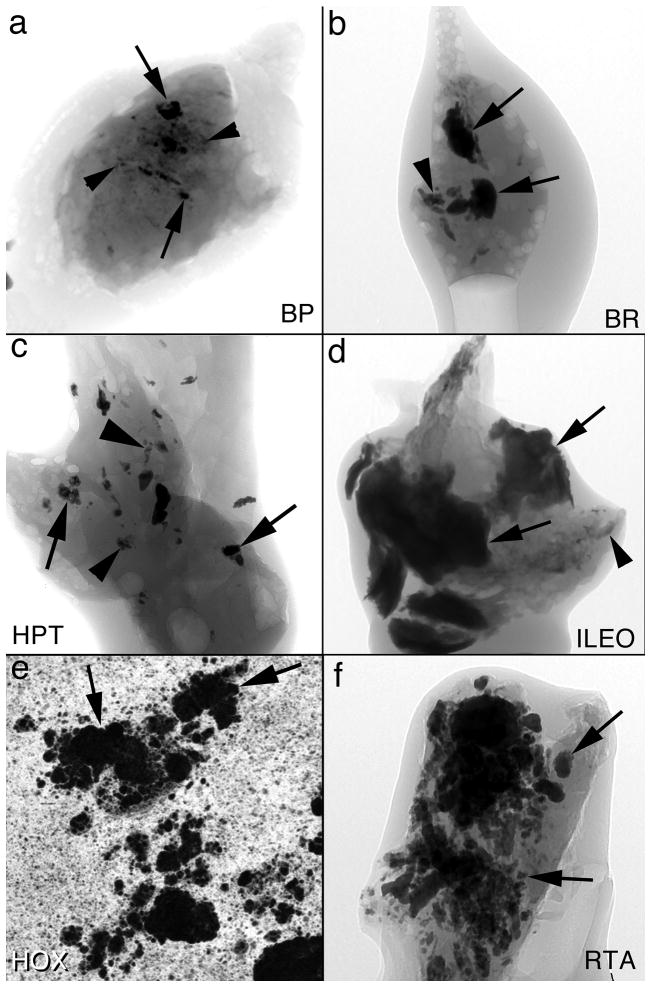
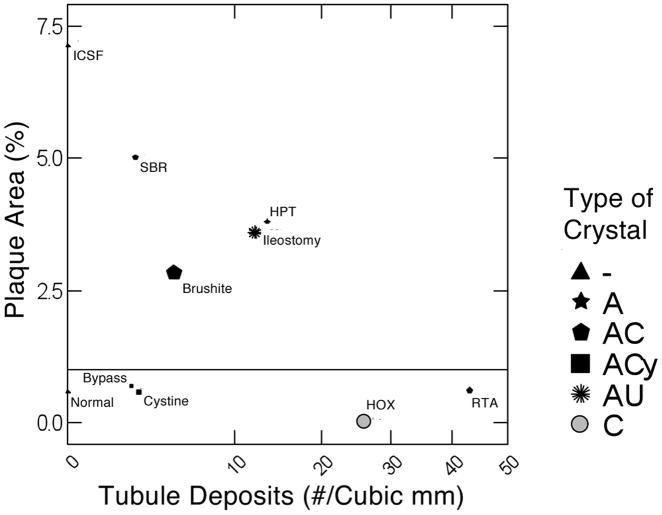
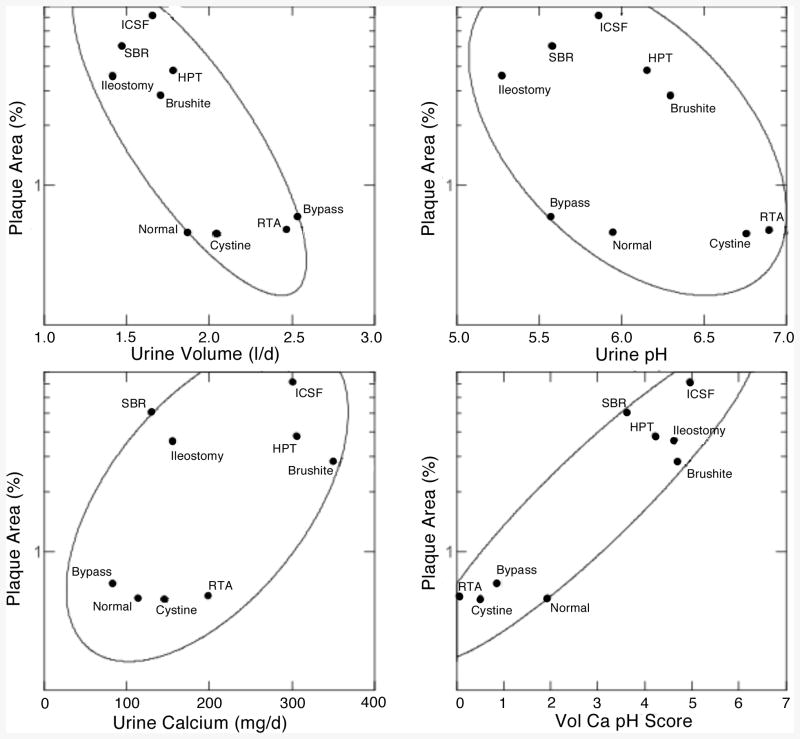
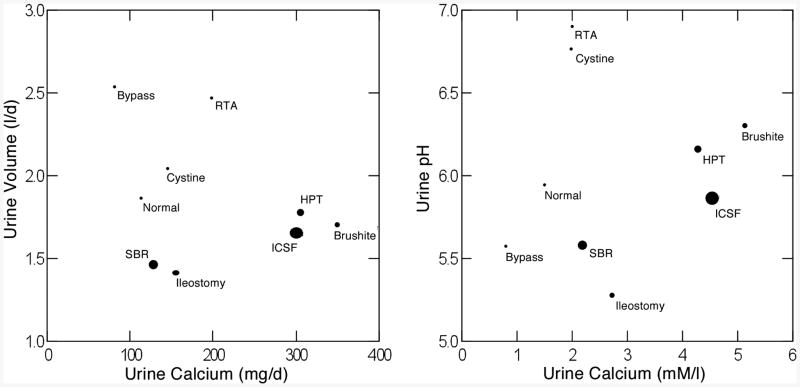
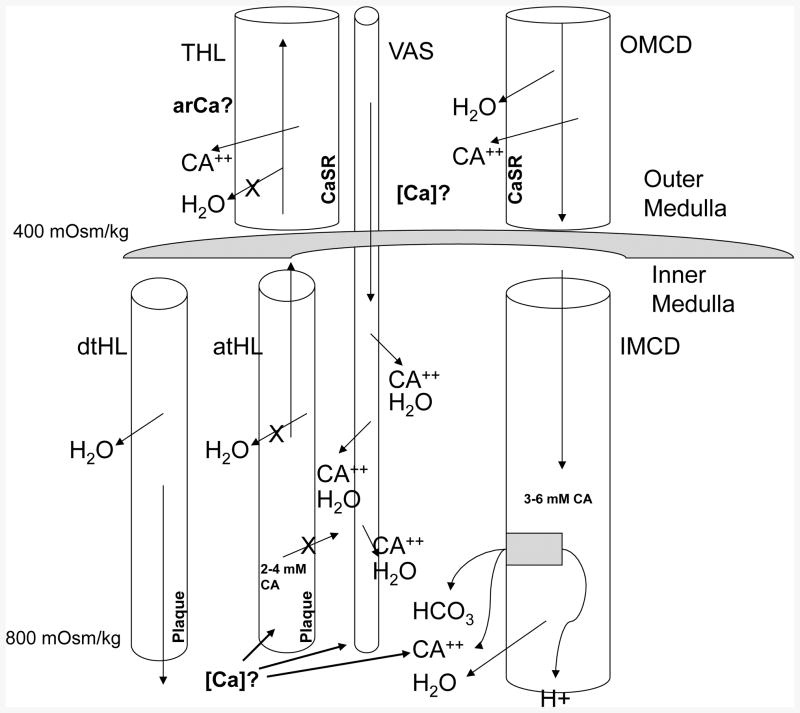
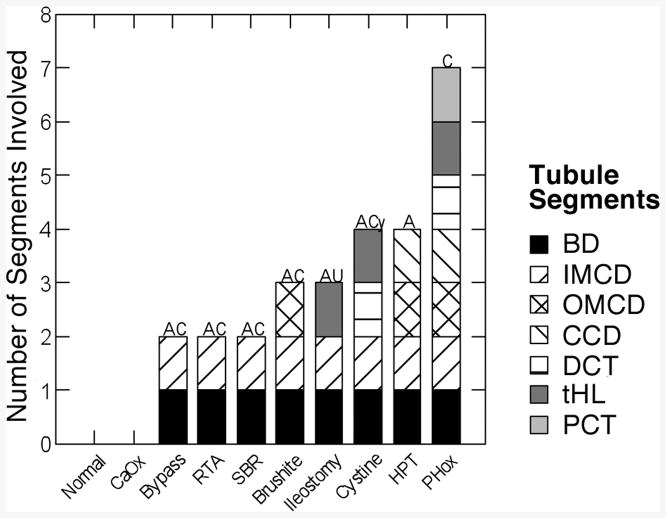
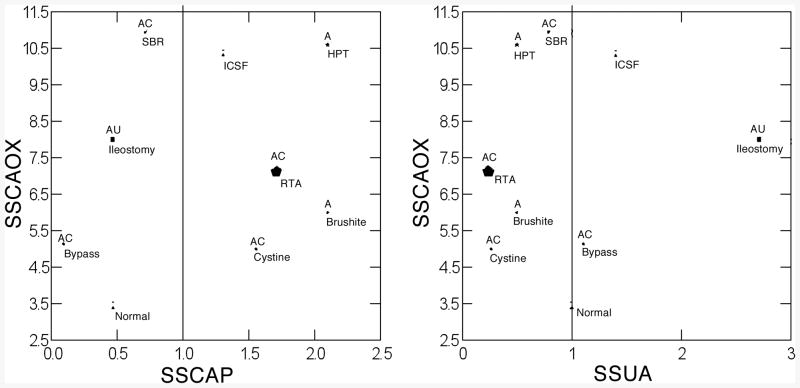
Data concerning nine forms of human stone disease, along with observations on normal people give new insights into formation of interstitial apatite plaque and intra-tubular crystal deposits. In general, across multiple disease states, one can reproduce the same relationships between plaque abundance as is seen among patients within individual disease states, so that the link between plaque and high urine calcium excretion, and low urine volume and pH seems increasingly secure. From this, one can propose a specific model of plaque formation, susceptible to experimental test. In many diseases, formation of inner medullary collecting duct and Bellini duct deposits is compatible with simple crystallization driven by urine supersaturations; this is expected in that these segments contain tubule fluid quite close in composition to final urine. But in ileostomy, small bowel disease and obesity bypass patients, crystals found in deposits are not those expected: apatite and urates in deposits, despite formation of highly acidic urine. Also, this discrepancy suggests the possibility of divergence between bulk urine pH and pH of focal collecting ducts, a new kind of possibility that is susceptible to experimental test.
Figures
References
-
- Evan AP, Coe FL, Lingeman JE, et al. Anat Rec. Vol. 290. Hoboken: 2007. Mechanism of formation of human calcium oxalate renal stones on Randall's plaque; pp. 1315–1323. - PubMed
-
- Kuo RL, Lingeman JE, Evan AP, et al. Urine calcium and volume predict coverage of renal papilla by Randall's plaque. Kidney Int. 2003;64:2150–2154. - PubMed
-
- Evan AP, Coe FL, Lingeman JE, et al. Renal crystal deposits and histopathology in patients with cystine stones. Kidney Int. 2006;69:2227–2235. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
