

Molecular characterization of intrahepatic and extrahepatic hepatitis B virus (HBV) reservoirs in patients on suppressive antiviral therapy
- PMID: 20626626
- PMCID: PMC4142495
- DOI: 10.1111/j.1365-2893.2010.01321.x
Molecular characterization of intrahepatic and extrahepatic hepatitis B virus (HBV) reservoirs in patients on suppressive antiviral therapy
Abstract
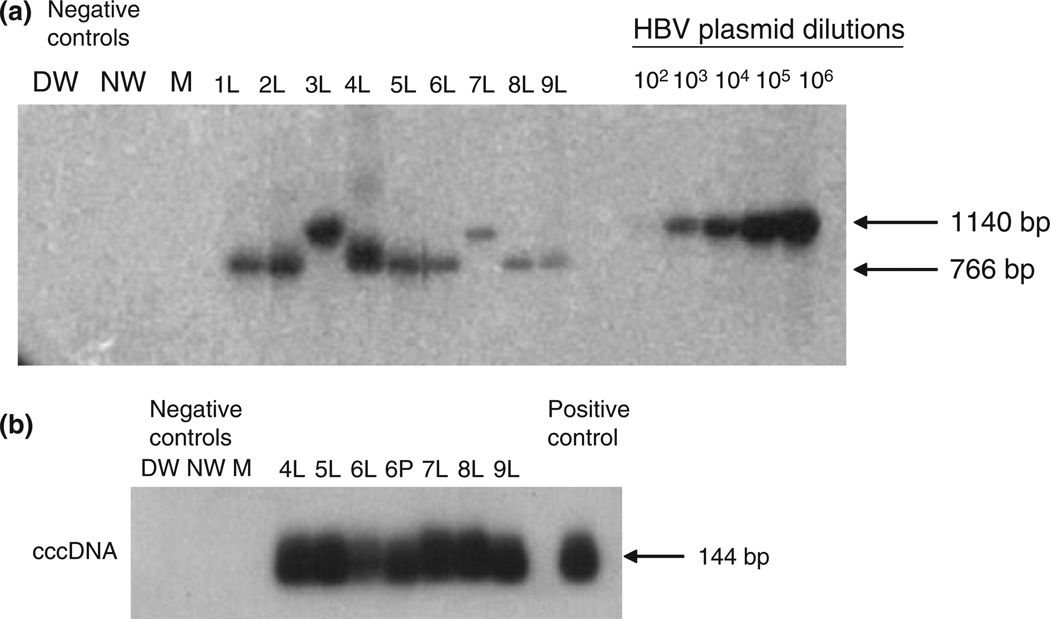
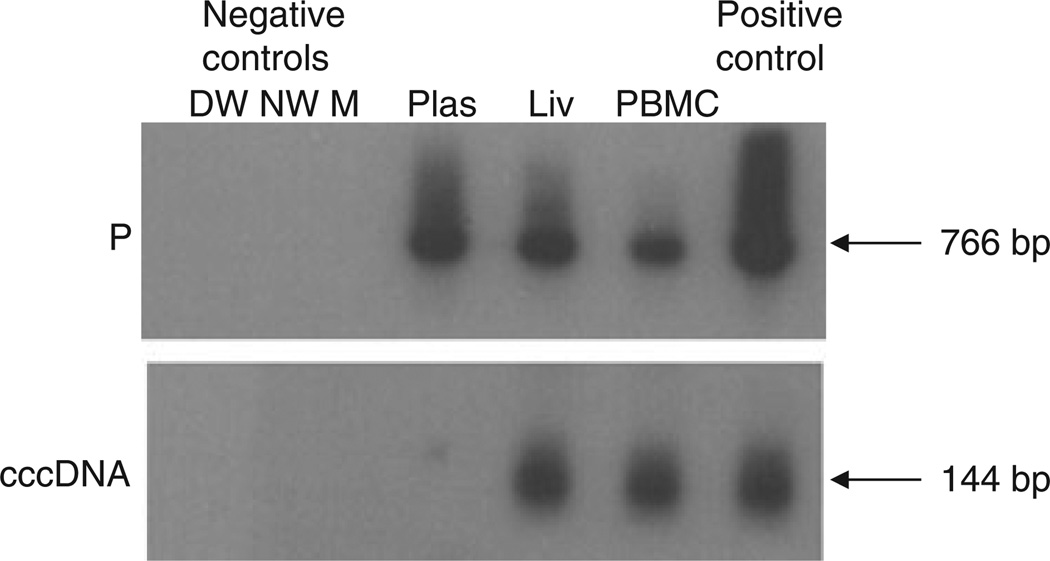
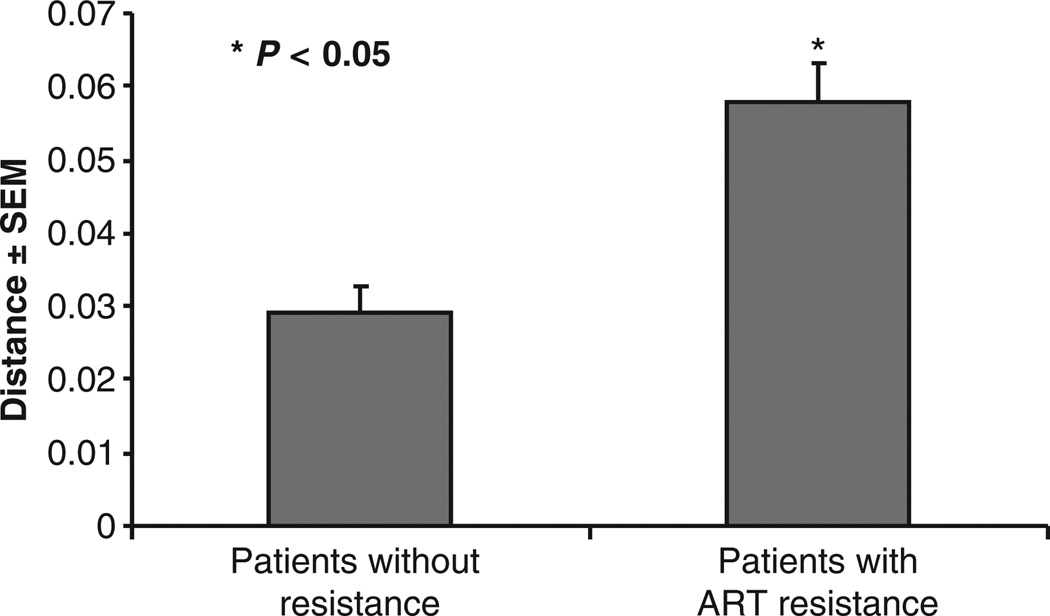
The hepatitis B virus (HBV) replicates via an error-prone reverse transcriptase generating potential drug-resistant quasispecies. The degree of HBV variability in liver vs peripheral blood mononuclear cells (PBMC) in patients on long-term suppressive antivirals is unclear. We characterized HBV replication, drug resistance and molecular diversity in patients with plasma HBV DNA undetectable by clinical assays. Explant liver (n=9), PBMC (n=6) and plasma (n=7) from nine such patients undergoing liver transplantation were evaluated for HBV genomes by sensitive PCR/nucleic acid hybridization assay. Cases with HBV DNA in liver and PBMC were tested for covalently closed circular DNA (HBV cccDNA). HBV polymerase (P) amplicons were cloned, sequenced and both P and overlapping surface (S) gene sequences were analysed. HBV DNA was detected in 43% (3/7) of plasma, 100% (9/9) of liver and 83% (5/6) of PBMC samples. HBV cccDNA was detected in all liver and one PBMC sample. Four patients had a clinical diagnosis of resistance. HBV P gene sequencing revealed 100% wild type (wt) in plasma (2/2), 83% wt in PBMC (5/6) but livers of 3/9 (33%) contained wt and 6/9 (66%) carried resistance to lamivudine and/or adefovir. The translated S gene revealed no changes affecting HBV antigenicity. Sequences from livers with antiviral resistant mutants revealed greater interpatient quasispecies diversity. Despite apparent HBV suppression, the liver continues to support HBV replication and extrahepatic HBV can be detected. PBMC may be a sanctuary for wt virus during antiviral therapy, while the liver harbours more drug-resistant viruses. Drug resistance correlates with intrahepatic viral diversity.
© 2010 Blackwell Publishing Ltd.
Figures

References
-
- Nassal M. Hepatitis B viruses: reverse transcription a different way. Virus Res. 2008;134(1–2):235–249. - PubMed
-
- Stuyver LJ, Locarnini SA, Lok A, et al. Nomenclature for antiviral-resistant human hepatitis B virus mutations in the polymerase region. Hepatology. 2001;33(3):751–757. - PubMed
-
- Lok AS, Lai CL, Leung N, et al. Long-term safety of lamivudine treatment in patients with chronic hepatitis B. Gastroenterology. 2003;125(6):1714–1722. - PubMed
-
- Bartholomeusz A, Locarnini S. Hepatitis B virus mutations associated with antiviral therapy. J Med Virol. 2006;78(Suppl. 1):S52–S55. - PubMed
-
- Sheldon J, Soriano V. Hepatitis B virus escape mutants induced by antiviral therapy. J Antimicrob Chemother. 2008;61(4):766–768. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
