

Updating the evidence for the role of corticosteroids in severe sepsis and septic shock: a Bayesian meta-analytic perspective
- PMID: 20626892
- PMCID: PMC2945102
- DOI: 10.1186/cc9182
Updating the evidence for the role of corticosteroids in severe sepsis and septic shock: a Bayesian meta-analytic perspective
Abstract
Introduction: Current low (stress) dose corticosteroid regimens may have therapeutic advantage in severe sepsis and septic shock despite conflicting results from two landmark randomised controlled trials (RCT). We systematically reviewed the efficacy of corticosteroid therapy in severe sepsis and septic shock.
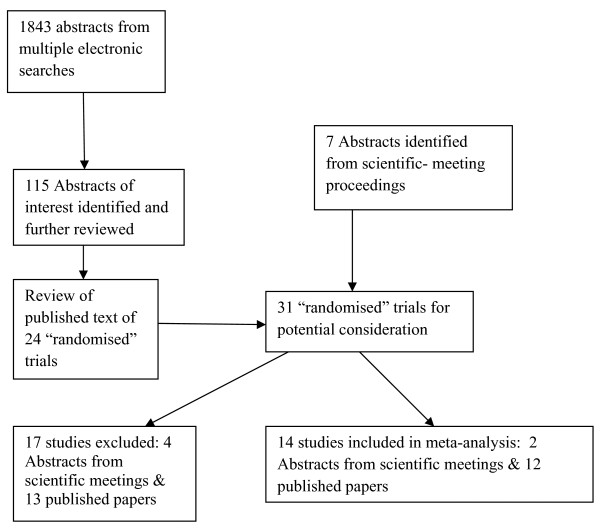
Methods: RCTs were identified (1950-September 2008) by multiple data-base electronic search (MEDLINE via OVID, OVID PreMedline, OVID Embase, Cochrane Central Register of Controlled trials, Cochrane database of systematic reviews, Health Technology Assessment Database and Database of Abstracts of Reviews of Effects) and hand search of references, reviews and scientific society proceedings. Three investigators independently assessed trial inclusion and data extraction into standardised forms; differences resolved by consensus.
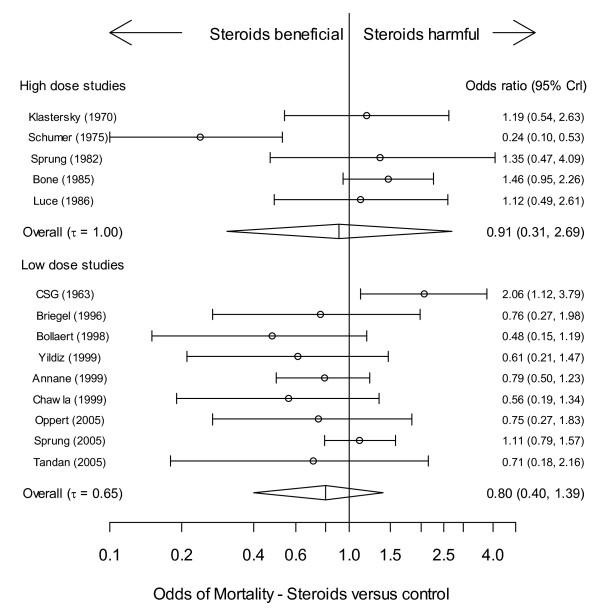
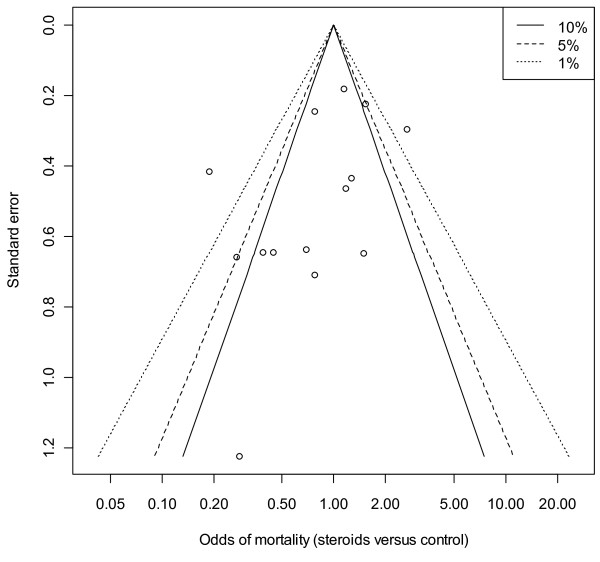
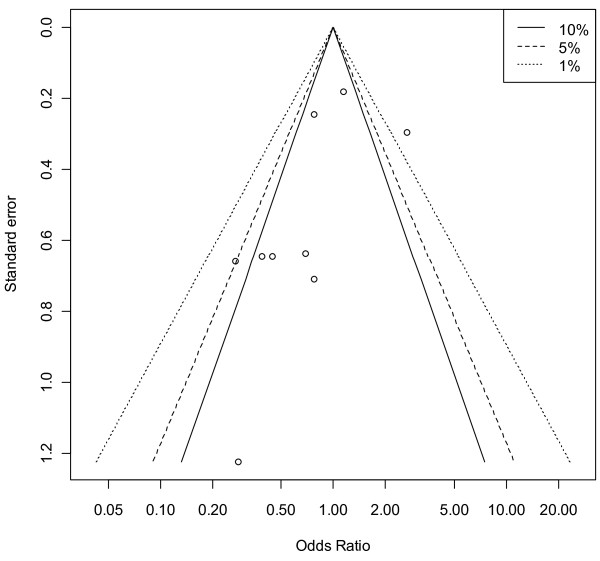
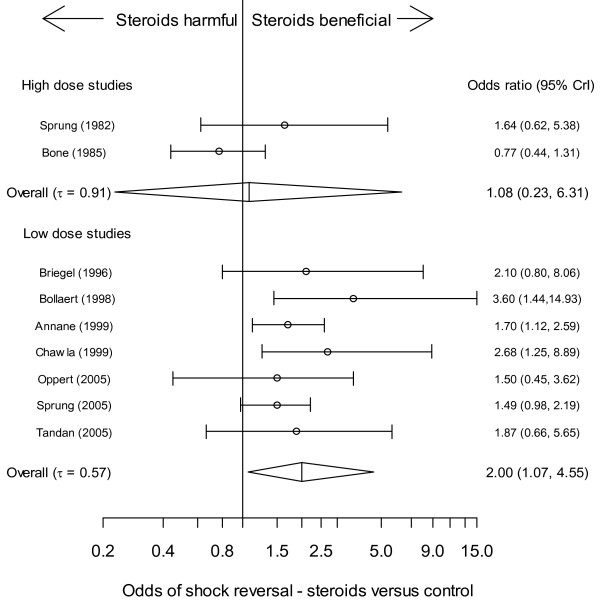
Results: Corticosteroid efficacy, compared with control, for hospital-mortality, proportion of patients experiencing shock-resolution, and infective and non-infective complications was assessed using Bayesian random-effects models; expressed as odds ratio (OR, (95% credible-interval)). Bayesian outcome probabilities were calculated as the probability (P) that OR ≥1. Fourteen RCTs were identified. High-dose (>1000 mg hydrocortisone (equivalent) per day) corticosteroid trials were associated with a null (n = 5; OR 0.91(0.31-1.25)) or higher (n = 4, OR 1.46(0.73-2.16), outlier excluded) mortality probability (P = 42.0% and 89.3%, respectively). Low-dose trials (<1000 mg hydrocortisone per day) were associated with a lower (n = 9, OR 0.80(0.40-1.39); n = 8 OR 0.71(0.37-1.10), outlier excluded) mortality probability (20.4% and 5.8%, respectively). OR for shock-resolution was increased in the low dose trials (n = 7; OR 1.20(1.07-4.55); P = 98.2%). Patient responsiveness to corticotrophin stimulation was non-determinant. A high probability of risk-related treatment efficacy (decrease in log-odds mortality with increased control arm risk) was identified by metaregression in the low dose trials (n = 9, slope coefficient -0.49(-1.14, 0.27); P = 92.2%). Odds of complications were not increased with corticosteroids.
Conclusions: Although a null effect for mortality treatment efficacy of low dose corticosteroid therapy in severe sepsis and septic shock was not excluded, there remained a high probability of treatment efficacy, more so with outlier exclusion. Similarly, although a null effect was not excluded, advantageous effects of low dose steroids had a high probability of dependence upon patient underlying risk. Low dose steroid efficacy was not demonstrated in corticotrophin non-responders. Further large-scale trials appear mandated.
Figures
References
-
- Weitzman S, Berger S. Clinical trial design in studies of corticosteroids for bacterial infections. Ann Intern Med. 1974;81:36–42. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
