

Regional variation in health care intensity and treatment practices for end-stage renal disease in older adults
- PMID: 20628131
- PMCID: PMC3477643
- DOI: 10.1001/jama.2010.924
Regional variation in health care intensity and treatment practices for end-stage renal disease in older adults
Abstract
Context: An increasing number of older adults are being treated for end-stage renal disease (ESRD) with long-term dialysis.
Objectives: To determine how ESRD treatment practices for older adults vary across regions with differing end-of-life intensity of care.
Design, setting, and participants: Retrospective observational study using a national ESRD registry to identify a cohort of 41,420 adults (of white or black race), aged 65 years or older, who started long-term dialysis or received a kidney transplant between June 1, 2005, and May 31, 2006. Regional end-of-life intensity of care was defined using an index from the Dartmouth Atlas of Healthcare.
Main outcome measures: Incidence of treated ESRD (dialysis or transplant), preparedness for ESRD (under the care of a nephrologist, having a fistula [vs graft or catheter] at time of hemodialysis initiation), and end-of-life care practices.
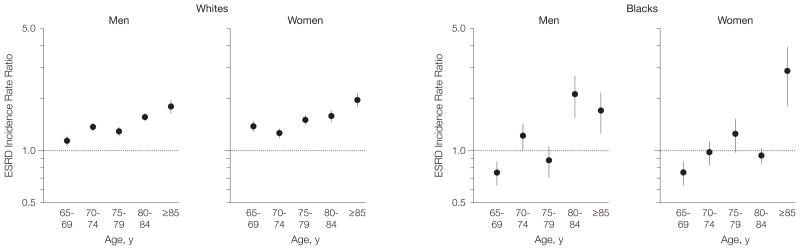
Results: Among whites, the incidence of ESRD was progressively higher in regions with greater intensity of care and this trend was most pronounced at older ages. Among blacks, a similar relationship was present only at advanced ages (men aged > or = 80 years and women aged > or = 85 years). Patients living in regions in the highest compared with lowest quintile of end-of-life intensity of care were less likely to be under the care of a nephrologist before the onset of ESRD (62.3% [95% confidence interval {CI}, 61.3%-63.3%] vs 71.1% [95% CI, 69.9%-72.2%], respectively) and less likely to have a fistula (vs graft or catheter) at the time of hemodialysis initiation (11.2% [95% CI, 10.6%-11.8%] vs 16.9% [95% CI, 15.9%-17.8%]). Among patients who died within 2 years of ESRD onset (n = 21,190), those living in regions in the highest compared with lowest quintile of end-of-life intensity of care were less likely to have discontinued dialysis before death (22.2% [95% CI, 21.1%-23.4%] vs 44.3% [95% CI, 42.5%-46.1%], respectively), less likely to have received hospice care (20.7% [95% CI, 19.5%-21.9%] vs 33.5% [95% CI, 31.7%-35.4%]), and more likely to have died in the hospital (67.8% [95% CI, 66.5%-69.1%] vs 50.3% [95% CI, 48.5%-52.1%]). These differences persisted in adjusted analyses.
Conclusion: There are pronounced regional differences in treatment practices for ESRD in older adults that are not explained by differences in patient characteristics.
Figures


References
-
- Fisher ES, Wennberg DE, Stukel TA, et al. The implications of regional variations in Medicare spending, part 1. Ann Intern Med. 2003;138(4):273–287. - PubMed
-
- US Renal Data System. [Accessed May 24, 2010.];US Renal Data System Web site. http:\\www.usrds.org.
-
- Mau LW, Liu J, Qiu Y, et al. Trends in patient characteristics and first-year medical costs of older incident hemodialysis patients, 1995–2005. Am J Kidney Dis. 2010;55(3):549–557. - PubMed
-
- Kurella M, Covinsky KE, Collins AJ, Chertow GM. Octogenarians and nonagenarians starting dialysis in the United States. Ann Intern Med. 2007;146(3):177–183. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
