

Multi-centre phase II clinical trial of yttrium-90 resin microspheres alone in unresectable, chemotherapy refractory colorectal liver metastases
- PMID: 20628388
- PMCID: PMC2920024
- DOI: 10.1038/sj.bjc.6605770
Multi-centre phase II clinical trial of yttrium-90 resin microspheres alone in unresectable, chemotherapy refractory colorectal liver metastases
Abstract
Background: This multi-centre phase II clinical trial is the first prospective evaluation of radioembolisation of patients with colorectal liver metastases (mCRC) who failed previous oxaliplatin- and irinotecan-based systemic chemotherapy regimens.
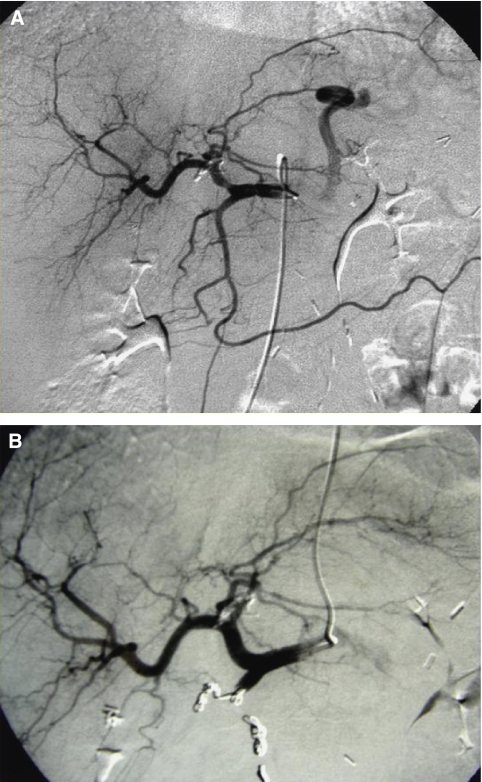
Methods: Eligible patients had adequate hepatic, haemopoietic and renal function, and an absence of major hepatic vascular anomalies and hepato-pulmonary shunting. Gastroduodenal and right gastric arteries were embolised before hepatic arterial administration of yttrium-90 resin microspheres (median activity, 1.7 GBq; range, 0.9-2.2).
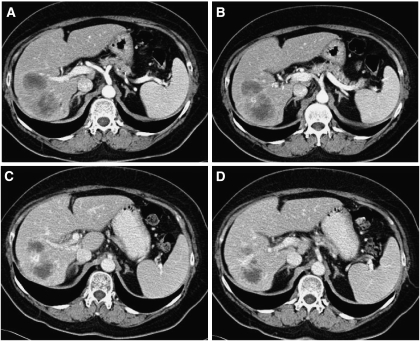
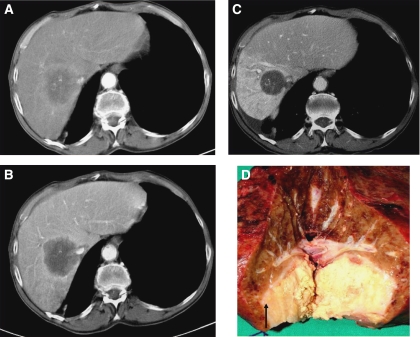
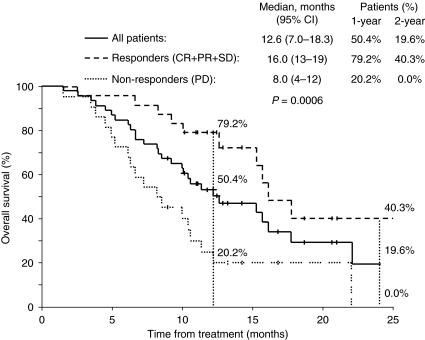
Results: Of 50 eligible patients, 38 (76%) had received > or =4 lines of chemotherapy. Most presented with synchronous disease (72%), >4 hepatic metastases (58%), 25-50% replacement of total liver volume (60%) and bilateral spread (70%). Early and intermediate (>48 h) WHO G1-2 adverse events (mostly fever and pain) were observed in 16 and 22% of patients respectively. Two died due to renal failure at 40 days or liver failure at 60 days respectively. By intention-to-treat analysis using Response Evaluation Criteria in Solid Tumours, 1 patient (2%) had a complete response, 11 (22%) partial response, 12 (24%) stable disease, 22 (44%) progressive disease; 4 (8%) were non-evaluable. Median overall survival was 12.6 months (95% CI, 7.0-18.3); 2-year survival was 19.6%.
Conclusion: Radioembolisation produced meaningful response and disease stabilisation in patients with advanced, unresectable and chemorefractory mCRC.
Figures
References
-
- A’Hern RP (2001) Sample size tables for exact single-stage phase II designs. Stat Med 20: 859–866 - PubMed
-
- Alberts SR, Roh MS, Mahoney MR, O’Connell MJ, Nagorney DM, Wagman L, Smyrk TC, Weiland TL, Lai LL, Schwarz RE, Molina R, Dentchev T, Bolton JS (2010) Alternating systemic and hepatic artery infusion therapy for resected liver metastases from colorectal cancer: a North Central Cancer Treatment Group (NCCTG)/National Surgical Adjuvant Breast and Bowel Project (NSABP) phase II intergroup trial, N9945/CI-66. J Clin Oncol 28: 853–858 - PMC - PubMed
-
- Atassi B, Bangash AK, Bahrani A, Pizzi G, Lewandowski RJ, Ryu RK, Sato KT, Gates VL, Mulcahy MF, Kulik L, Miller F, Yaghmai V, Murthy R, Larson A, Omary RA, Salem R (2008) Multimodality imaging following 90Y radioembolization: a comprehensive review and pictorial essay. Radiographics 28: 81–99 - PubMed
-
- Bipat S, van Leeuwen MS, Ijzermans JN, Comans EF, Planting AS, Bossuyt PM, Greve JW, Stoker J (2007) Evidence-base guideline on management of colorectal liver metastases in the Netherlands. Neth J Med 65: 5–14 - PubMed
-
- Bouchahda M, Adam R, Giacchetti S, Castaing D, Brezault-Bonnet C, Hauteville D, Innominato PF, Focan C, Machover D, Lévi F (2009) Rescue chemotherapy using multidrug chronomodulated hepatic arterial infusion for patients with heavily pretreated metastatic colorectal cancer. Cancer 115: 4990–4999 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
