

Effect of trandolapril on regression of retinopathy in hypertensive patients with type 2 diabetes: a prespecified analysis of the benedict trial
- PMID: 20628590
- PMCID: PMC2901608
- DOI: 10.1155/2010/106384
Effect of trandolapril on regression of retinopathy in hypertensive patients with type 2 diabetes: a prespecified analysis of the benedict trial
Abstract
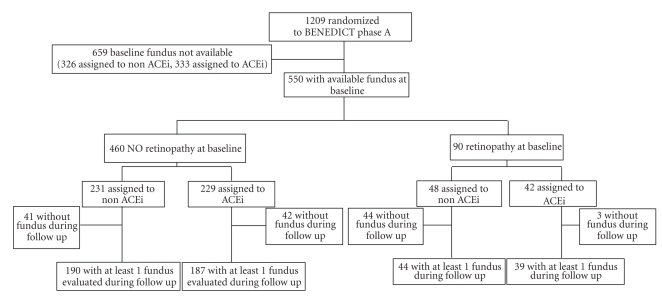
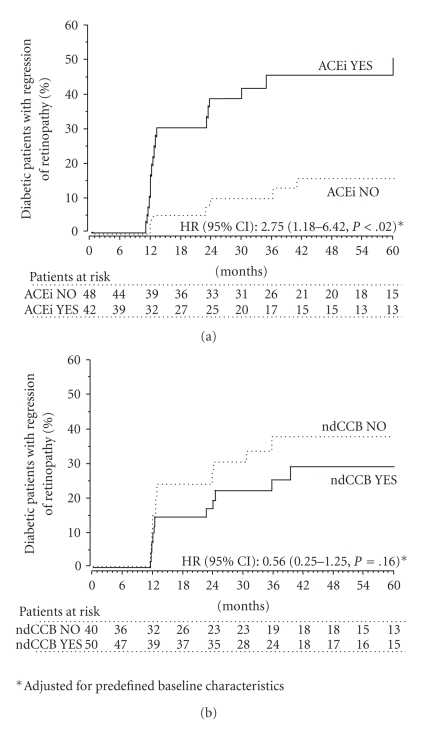
Background. The effect of angiotensin converting enzyme inhibitors (ACEi) on regression of retinopathy in type 2 diabetics is still ill defined. Methods. We compared the incidence of retinopathy regression in 90 hypertensive type 2 diabetics randomized to at least 3-year blinded ACEi with trandolapril (2 mg/day) or non-ACEi therapy who had preproliferative or proliferative retinopathy at baseline. Results. Over a median (interquartile range) follow-up period of 35.8 (12.4-60.7) months, retinopathy regressed in 27 patients (30.0%). Regression occurred in 18 of 42 patients (42.9%) on ACEi and in 9 of 48 (18.8%) on non-ACEi therapy (adjusted for predefined baseline covariates HR (95% CI): 2.75 (1.18-6.42), P = .0193). Concomitant treatment with or without Non-Dihydropyridine Calcium Channel Blockers (ndCCBs) did not appreciably affect the incidence of retinopathy regression. Conclusions. Unlike ndCCB, ACEi therapy may have an additional effect to that of intensified BP and metabolic control in promoting regression of diabetic retinopathy.
Figures
References
-
- Keen H, Lee ET, Russell D, Miki E, Bennett PH, Lu M. The appearance of retinopathy and progression to proliferative retinopathy: the WHO Multinational Study of Vascular Disease in Diabetes. Diabetologia. 2001;44(supplement 2):S22–S30. - PubMed
-
- Stratton IM, Kohner EM, Aldington SJ, et al. UKPDS 50: risk factors for incidence and progression of retinopathy in type II diabetes over 6 years from diagnosis. Diabetologia. 2001;44(2):156–163. - PubMed
-
- Ruggenenti P, Fassi A, Ilieva AP, et al. Preventing microalbuminuria in type 2 diabetes. New England Journal of Medicine. 2004;351(19):1941–1951. - PubMed
-
- Kohner EM, Porta M. Screening for Diabetic Retinopathy in Europe: A Field Guide-Book. Copenhagen, Denmark: WHO; 1992.
-
- Parvanova A, Iliev I, Filipponi M, et al. Insulin resistance and proliferative retinopathy: a cross-sectional, case-control study in 115 patients with type 2 diabetes. Journal of Clinical Endocrinology and Metabolism. 2004;89(9):4371–4376. - PubMed
LinkOut - more resources
Full Text Sources
