

Ambulatory-based education in internal medicine: current organization and implications for transformation. Results of a national survey of resident continuity clinic directors
- PMID: 20628830
- PMCID: PMC3024101
- DOI: 10.1007/s11606-010-1437-3
Ambulatory-based education in internal medicine: current organization and implications for transformation. Results of a national survey of resident continuity clinic directors
Abstract
Background: Many have called for ambulatory training redesign in internal medicine (IM) residencies to increase primary care career outcomes. Many believe dysfunctional, clinic environments are a key barrier to meaningful ambulatory education, but little is actually known about the educational milieu of continuity clinics nationwide.
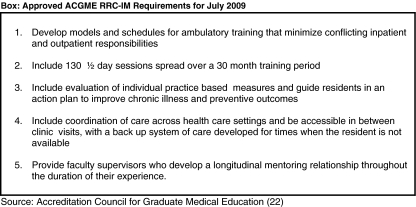
Objective: We wished to describe the infrastructure and educational milieu at resident continuity clinics and assess clinic readiness to meet new IM-RRC requirements.
Design: National survey of ACGME accredited IM training programs.
Participants: Directors of academic and community-based continuity clinics.
Results: Two hundred and twenty-one out of 365 (62%) of clinic directors representing 49% of training programs responded. Wide variation amongst continuity clinics in size, structure and educational organization exist. Clinics below the 25th percentile of total clinic sessions would not meet RRC-IM requirements for total number of clinic sessions. Only two thirds of clinics provided a longitudinal mentor. Forty-three percent of directors reported their trainees felt stressed in the clinic environment and 25% of clinic directors felt overwhelmed.
Limitations: The survey used self reported data and was not anonymous. A slight predominance of larger clinics and university based clinics responded. Data may not reflect changes to programs made since 2008.
Conclusions: This national survey demonstrates that the continuity clinic experience varies widely across IM programs, with many sites not yet meeting new ACGME requirements. The combination of disadvantaged and ill patients with inadequately resourced clinics, stressed residents, and clinic directors suggests that many sites need substantial reorganization and institutional commitment.New paradigms, encouraged by ACGME requirement changes such as increased separation of inpatient and outpatient duties are needed to improve the continuity clinic experience.
Figures
Comment in
-
Primary care and primary care training: mirror images.J Gen Intern Med. 2011 Jan;26(1):5-7. doi: 10.1007/s11606-010-1561-0. J Gen Intern Med. 2011. PMID: 21063799 Free PMC article. No abstract available.
References
-
- Weinberger SE, Smith LG, Collier VU. Education Committee of the American College of Physicians. Redesigning training for internal medicine. Ann Intern Med. 2006;144:927–32. - PubMed
-
- Meyers FJ, Weinberger SE, Fitzgibbons JP, Glassroth J, Duffy FD. Clayton CP; Alliance for Academic Internal Medicine Education Redesign Task Force. Redesigning residency training in internal medicine: the consensus report of the Alliance for Academic Internal Medicine Education Redesign Task Force. Acad Med. 2007;82:1211–19. doi: 10.1097/ACM.0b013e318159d010. - DOI - PubMed
-
- Fitzgibbons JP, Bordley DR, Berkowitz LR, Miller BW, Henderson MC. Redesigning residency education in internal medicine: A position paper from the Association of Program Directors in Internal Medicine. Ann Intern Med. 2006;144:920–26. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
