

Efficacy and safety of irbesartan/HCTZ in severe hypertension according to cardiometabolic factors
- PMID: 20629810
- PMCID: PMC8673052
- DOI: 10.1111/j.1751-7176.2010.00294.x
Efficacy and safety of irbesartan/HCTZ in severe hypertension according to cardiometabolic factors
Abstract
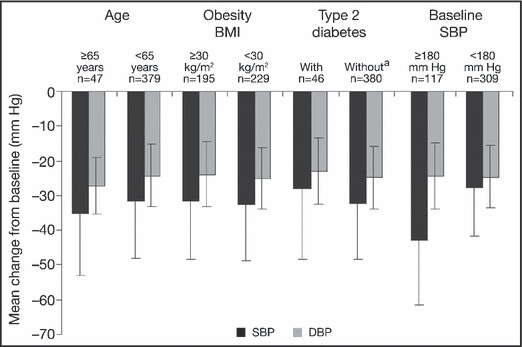
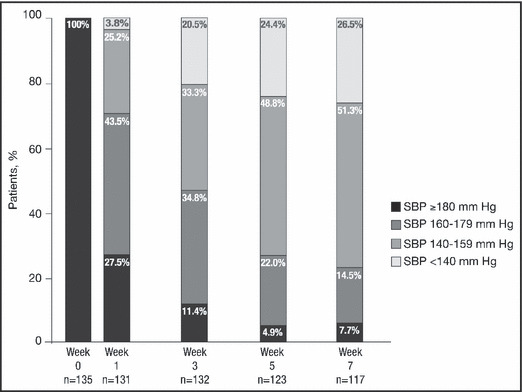
This post hoc analysis of a 7-week, randomized, double-blind trial evaluated the efficacy and safety of initial irbesartan/hydrochlorothiazide treatment in 468 patients with severe, uncontrolled, hypertension (diastolic blood pressure [DBP] > or =100 mm Hg) at high cardiovascular risk. Systolic blood pressure (SBP)/DBP reductions ranged from 28.0 to 42.9/22.9 to 27.2 mm Hg in patients with obesity, diabetes, baseline SBP > or =180 mm Hg, and in the elderly. Blood pressure control to <140/90 mm Hg in the age and obesity subgroups ranged from 32.1% to 39.2% while control to <130/80 mm Hg in patients with diabetes was 11.5%. After 1 week of therapy, 72.5% of patients no longer had SBP > or =180 mm Hg; by 7 weeks, 51.3% had SBP 140 to 159 mm Hg and 26.5% had SBP <140 mm Hg. Treatment was well tolerated regardless of the subgroup. No excess of prespecified events was noted. Thus, initial treatment with irbesartan/hydrochlorothiazide was rapidly effective in high-risk, difficult-to-treat, severely hypertensive patients.
Figures
References
-
- Zampaglione B, Pascale C, Marchisio M, et al. Hypertensive urgencies and emergencies. Prevalence and clinical presentation. Hypertension. 1996;27:144–147. - PubMed
-
- Effects of treatment on morbidity in hypertension. Results in patients with diastolic blood pressures averaging 115 through 129 mm Hg. JAMA. 1967;202:1028–1034. - PubMed
-
- Lewington S, Clarke R, Qizilbash N, et al. Age‐specific relevance of usual blood pressure to vascular mortality: a meta‐analysis of individual data for one million adults in 61 prospective studies. Lancet. 2002;360:1903–1913. - PubMed
-
- Anderson TW. Re‐examination of some of the Framingham blood‐pressure data. Lancet. 1978;2:1139–1141. - PubMed
-
- Mancia G, De Backer G, Dominiczak A, et al. 2007 Guidelines for the Management of Arterial Hypertension: The Task Force for the Management of Arterial Hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). J Hypertens. 2007;25:1105–1187. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
