

Lymphangioleiomyomatosis (LAM): molecular insights lead to targeted therapies
- PMID: 20630348
- PMCID: PMC3030250
- DOI: 10.1016/j.rmed.2010.03.017
Lymphangioleiomyomatosis (LAM): molecular insights lead to targeted therapies
Abstract
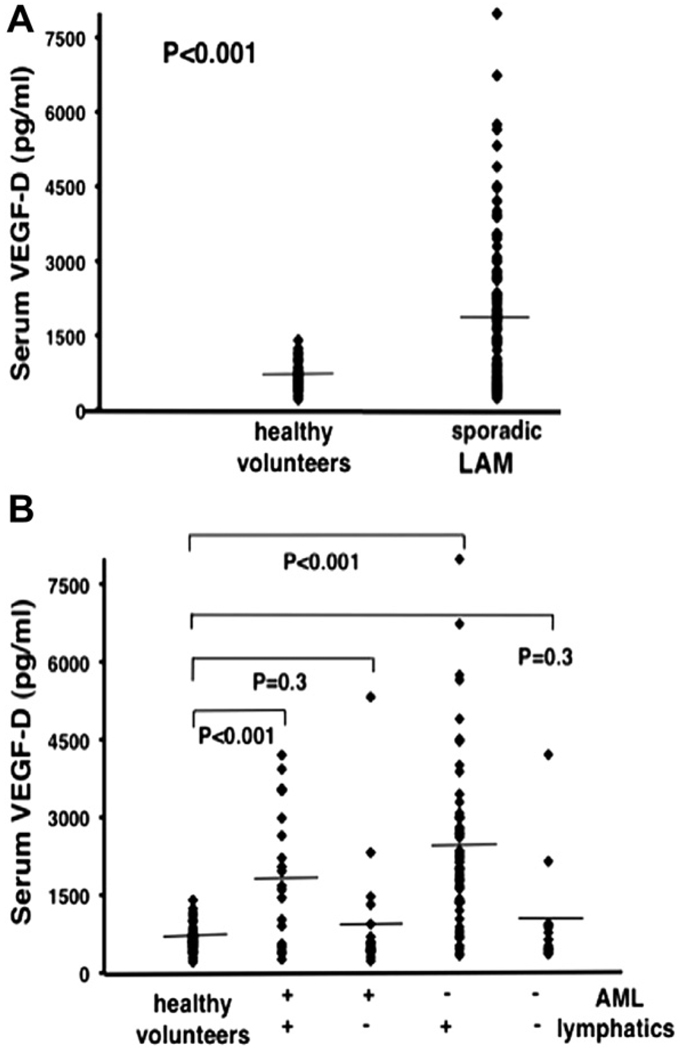
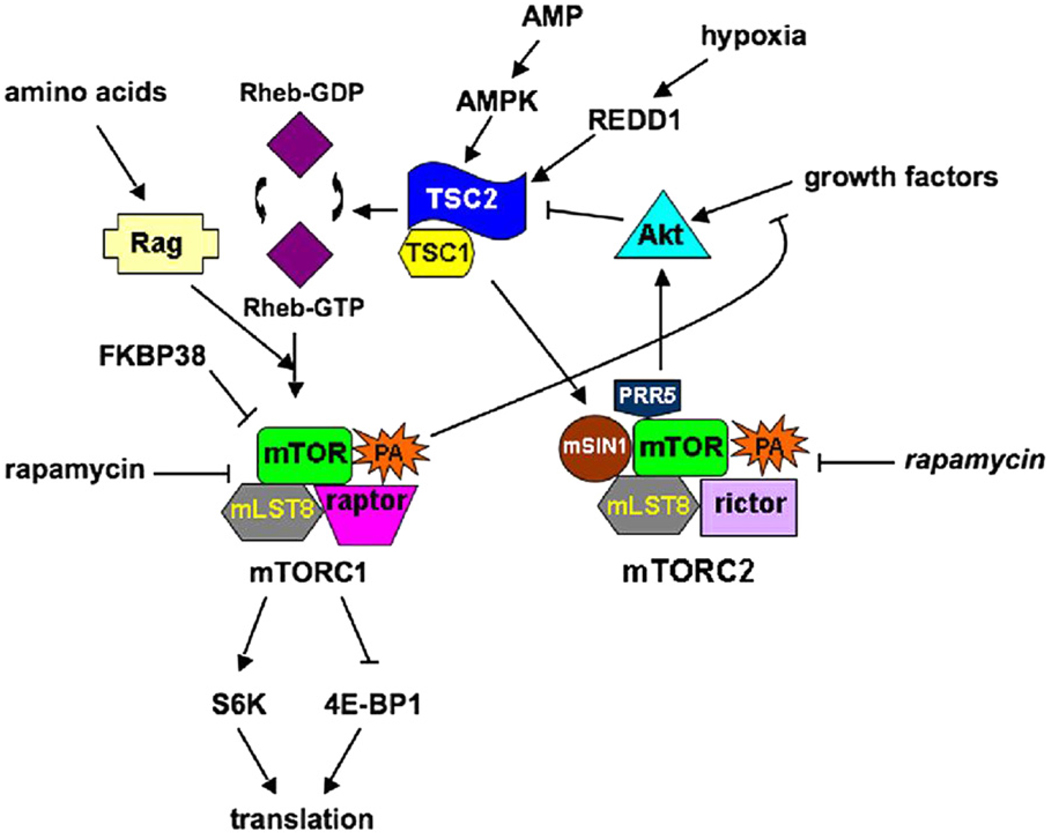
LAM is a rare lung disease, found primarily in women of childbearing age, characterized by cystic lung destruction and abdominal tumors (e.g., renal angiomyolipoma, lymphangioleiomyoma). The disease results from proliferation of a neoplastic cell, termed the LAM cell, which has mutations in either of the tuberous sclerosis complex (TSC) 1 or TSC2 genes. Molecular phenotyping of LAM patients resulted in the identification of therapeutic targets for drug trials. Loss of TSC gene function leads to activation of mammalian target of rapamycin (mTOR), and thereby, effects on cell size and number. The involvement of mTOR in LAM pathogenesis is the basis for initiation of therapeutic trials of mTOR inhibitors (e.g., sirolimus). Occurrence of LAM essentially entirely in women is consistent with the hypothesis that anti-estrogen agents might prevent disease progression (e.g., gonadotropin-releasing hormone analogues). Levels of urinary matrix metalloproteinases (MMPs) were elevated in LAM patients, and MMPs were found in LAM lung nodules. In part because of these observations, effects of doxycycline, an anti-MMP, and anti-angiogenic agent, are under investigation. The metastatic properties of LAM cells offer additional potential for targets. Thus, insights into the molecular and biological properties of LAM cells and molecular phenotyping of patients with LAM have led to clinical trials of targeted therapies. Funded by the Intramural Research Program, NIH/NHLBI.
Copyright (c) 2010. Published by Elsevier Ltd.
Conflict of interest statement
The authors have no financial conflicts of interest to disclose.
Figures
References
-
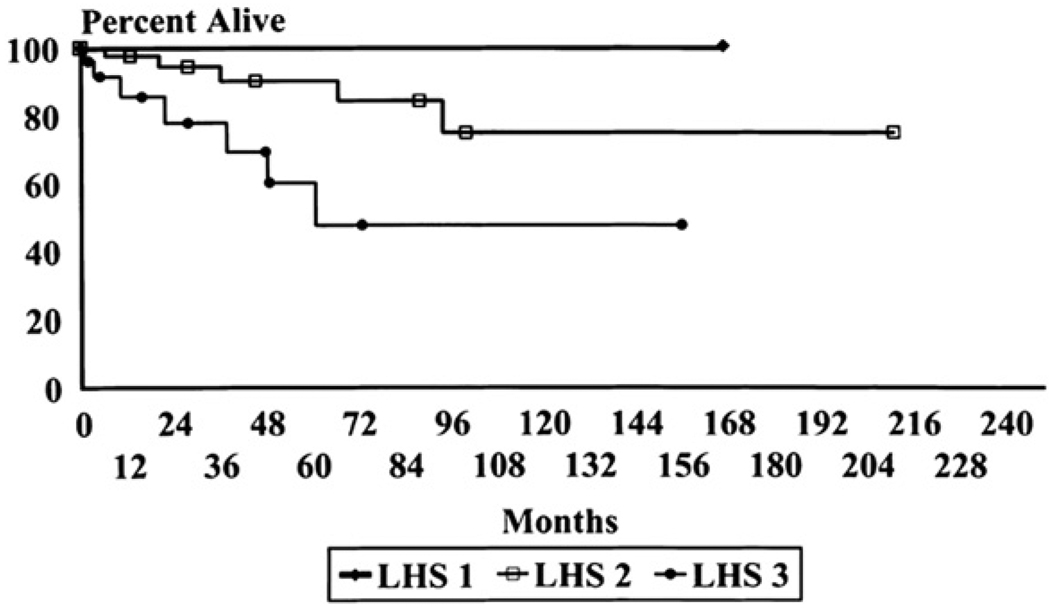
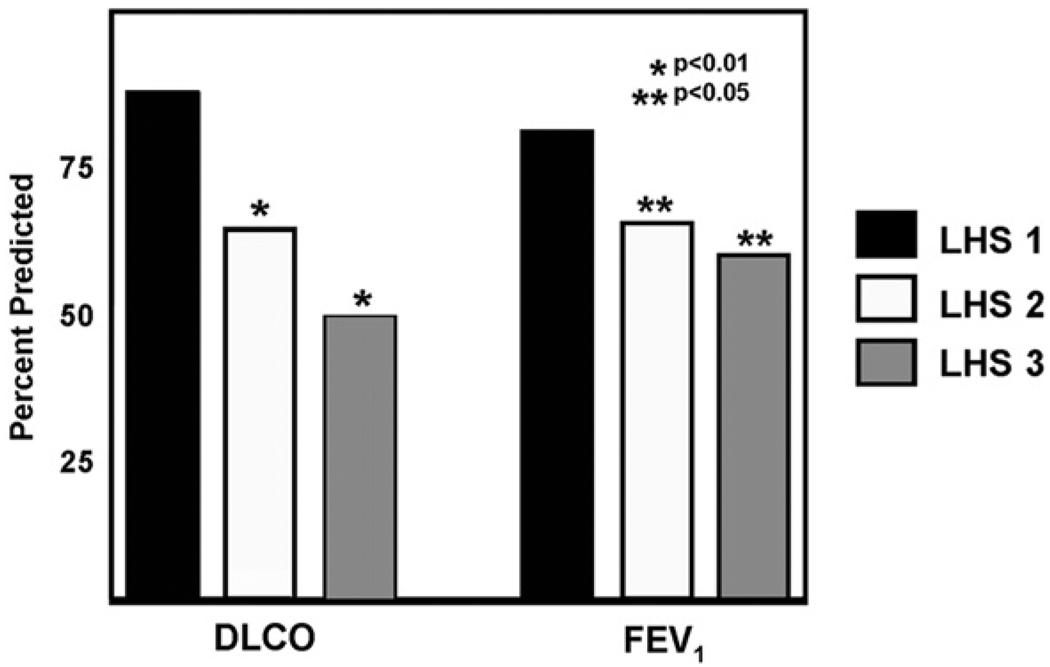
- Kitaichi M, Nishimura K, Itoh H, Izumi T. Pulmonary lymphangioleiomyomatosis: a report of 46 patients including a clinicopathologic study of prognostic factors. Am J Respir Crit Care Med. 1995 Feb;151(2 Pt 1):527–533. - PubMed
-
- Chu SC, Horiba K, Usuki J, Avila NA, Chen CC, Travis WD, et al. Comprehensive evaluation of 35 patients with lymphangioleiomyomatosis. Chest. 1999 Apr;115(4):1041–1052. - PubMed
-
- Urban T, Lazor R, Lacronique J, Murris M, Labrune S, Valeyre D, et al. Pulmonary lymphangioleiomyomatosis. A study of 69 patients. Groupe d’Etudes et de Recherche sur les Maladies “Orphelines” Pulmonaires (GERM“O”P) Medicine (Baltimore) 1999 Sep;78(5):321–337. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
