

Targeting the immune system in non-small-cell lung cancer: bridging the gap between promising concept and therapeutic reality
- PMID: 20630824
- PMCID: PMC3474196
- DOI: 10.3816/CLC.2010.n.029
Targeting the immune system in non-small-cell lung cancer: bridging the gap between promising concept and therapeutic reality
Abstract
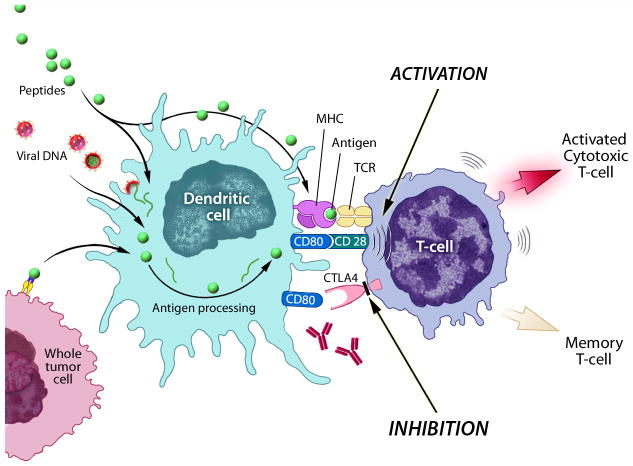
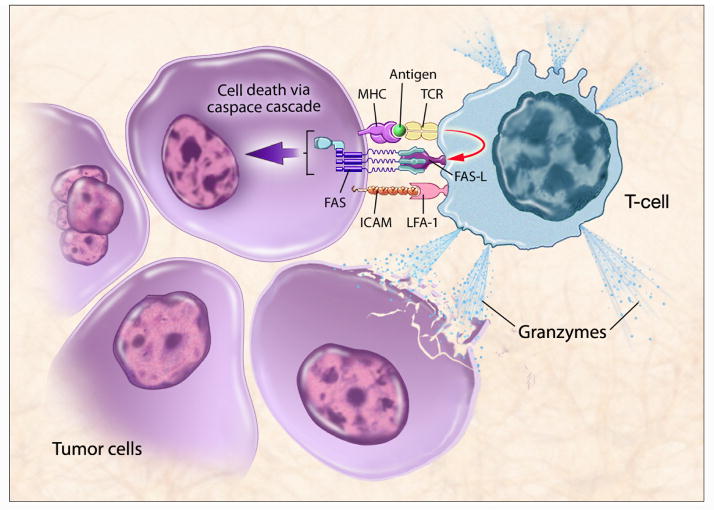
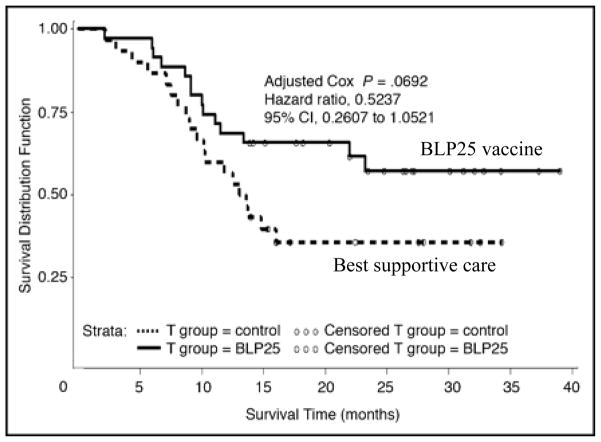
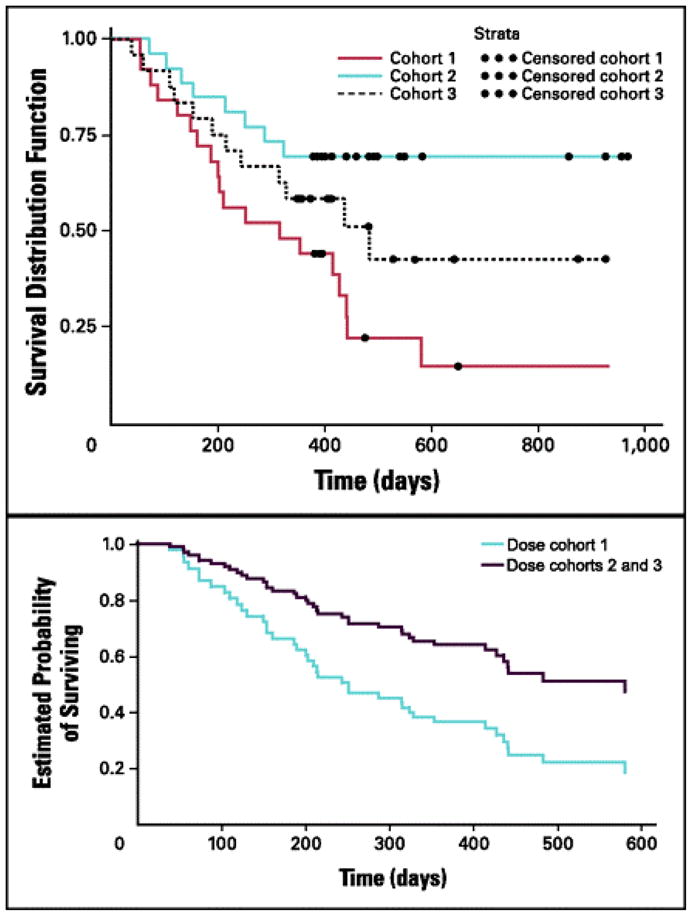
Developing effective immunotherapy for lung cancer is a daunting but hugely attractive challenge. Until recently, non-small-cell lung cancer (NSCLC) was thought of as a nonimmunogenic tumor, but there is now evidence highlighting the integral role played by both inflammatory and immunologic responses in lung carcinogenesis. Despite recent encouraging preclinical and phase I/II data, there are a paucity of phase III trials showing a clear clinical benefit for vaccines in lung cancer. There are many difficulties to overcome before the development of a successful therapy. Perhaps a measurable immune response may not translate into a clinically meaningful or radiologic response. Patient selection may also be a problem for ongoing clinical studies. The majority of trials for lung cancer vaccines are focused on patients with an advanced stage of the disease; however, the ideal candidates may be patients with a lower tumor burden and stage I or II disease. Selecting the exact antigens to target is also difficult. It will likely require multiple epitopes of a diverse set of genes restricted to multiple haplotypes to generate a truly effective vaccine that is able to overcome the various immunologic escape mechanisms that tumors use. This review discusses the most promising active immunotherapy using protein/peptide vaccines, whole cell vaccines, and dendritic cell vaccines and examines current phase I and II clinical trial data on some novel nonspecific immunomodulating agents.
Figures
References
-
- Cancer Facts & Figures. American Cancer Society; Atlanta, GA: 2006.
-
- Sugimura H, Nichols FC, Yang P, Allen MS, Cassivi SD, Deschamps C, Williams BA, Pairolero PC. Survival after recurrent nonsmall-cell lung cancer after complete pulmonary resection. Ann Thorac Surg. 2007;83:409–417. discussioin 417–408. - PubMed
-
- Shepherd FA, Dancey J, Ramlau R, Mattson K, Gralla R, O'Rourke M, Levitan N, Gressot L, Vincent M, Burkes R, Coughlin S, Kim Y, Berille J. Prospective randomized trial of docetaxel versus best supportive care in patients with non-small-cell lung cancer previously treated with platinum-based chemotherapy. J Clin Oncol. 2000;18:2095–2103. - PubMed
-
- Banchereau J, Steinman RM. Dendritic cells and the control of immunity. Nature. 1998;392:245–252. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
