

A novel syndrome of mandibular hypoplasia, deafness, and progeroid features associated with lipodystrophy, undescended testes, and male hypogonadism
- PMID: 20631028
- PMCID: PMC3050107
- DOI: 10.1210/jc.2010-0419
A novel syndrome of mandibular hypoplasia, deafness, and progeroid features associated with lipodystrophy, undescended testes, and male hypogonadism
Abstract
Context: Mandibuloacral dysplasia (MAD) is an autosomal recessive progeroid disorder associated with type A (partial) or B (generalized) lipodystrophy and is due to mutations in lamin A/C (LMNA) or zinc metalloproteinase (ZMPSTE24) genes.
Objective: The objective of the study was to report a novel syndrome with some overlapping features with MAD.
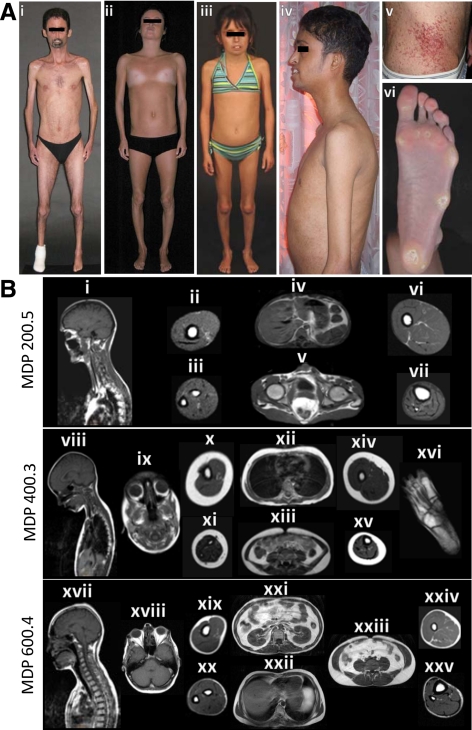
Results: We report seven patients with mandibular hypoplasia, deafness, progeroid features (MDP), and associated lipodystrophy. These patients have similar features to MAD patients such as hypoplastic mandible, beaked nose, stiff joints, and sclerodermatous skin. However, the patients did not harbor any disease causing variants in LMNA or ZMPSTE24 and showed distinct characteristics such as sensorineural hearing loss and absence of clavicular hypoplasia and acroosteolysis. All males with MDP had undescended testes and were hypogonadal. One adult female showed lack of breast development. Skinfold thickness, dual-energy X-ray absorptiometry and whole-body magnetic resonance imaging for body fat distribution revealed a lack of lipodystrophy in a prepubertal female but a progressive loss of sc fat presenting with partial lipodystrophy in young adults and generalized lipodystrophy in older patients.
Conclusions: Patients with MDP syndrome have a few overlapping but some distinct clinical features as compared with MAD, suggesting that it is a novel syndrome. The molecular basis of MDP syndrome remains to be elucidated.
Figures
References
-
- Simha V, Garg A 2002 Body fat distribution and metabolic derangements in patients with familial partial lipodystrophy associated with mandibuloacral dysplasia. J Clin Endocrinol Metab 87:776–785 - PubMed
-
- Freidenberg GR, Cutler DL, Jones MC, Hall B, Mier RJ, Culler F, Jones KL, Lozzio C, Kaufmann S 1992 Severe insulin resistance and diabetes mellitus in mandibuloacral dysplasia. Am J Dis Child 146:93–99 - PubMed
-
- Young LW, Radebaugh JF, Rubin P, Sensenbrenner JA, Fiorelli G, McKusick VA 1971 New syndrome manifested by mandibular hypoplasia, acroosteolysis, stiff joints and cutaneous atrophy (mandibuloacral dysplasia) in two unrelated boys. Birth Defects Orig Artic Ser 7:291–297 - PubMed
-
- Novelli G, Muchir A, Sangiuolo F, Helbling-Leclerc A, D'Apice MR, Massart C, Capon F, Sbraccia P, Federici M, Lauro R, Tudisco C, Pallotta R, Scarano G, Dallapiccola B, Merlini L, Bonne G 2002 Mandibuloacral dysplasia is caused by a mutation in LMNA-encoding lamin A/C. Am J Hum Genet 71:426–431 - PMC - PubMed
-
- Simha V, Agarwal AK, Oral EA, Fryns JP, Garg A 2003 Genetic and phenotypic heterogeneity in patients with mandibuloacral dysplasia-associated lipodystrophy. J Clin Endocrinol Metab 88:2821–2824 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Miscellaneous
