

Vorinostat and sorafenib increase CD95 activation in gastrointestinal tumor cells through a Ca(2+)-de novo ceramide-PP2A-reactive oxygen species-dependent signaling pathway
- PMID: 20631069
- PMCID: PMC2918282
- DOI: 10.1158/0008-5472.CAN-10-0999
Vorinostat and sorafenib increase CD95 activation in gastrointestinal tumor cells through a Ca(2+)-de novo ceramide-PP2A-reactive oxygen species-dependent signaling pathway
Abstract
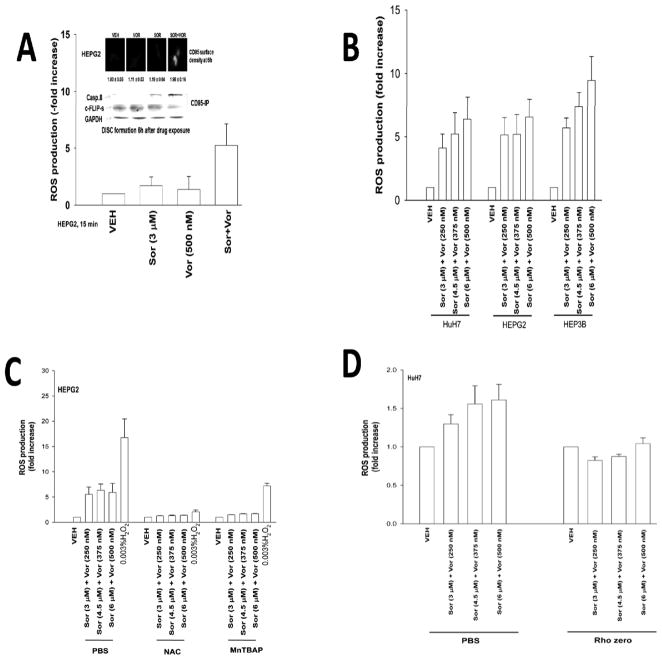
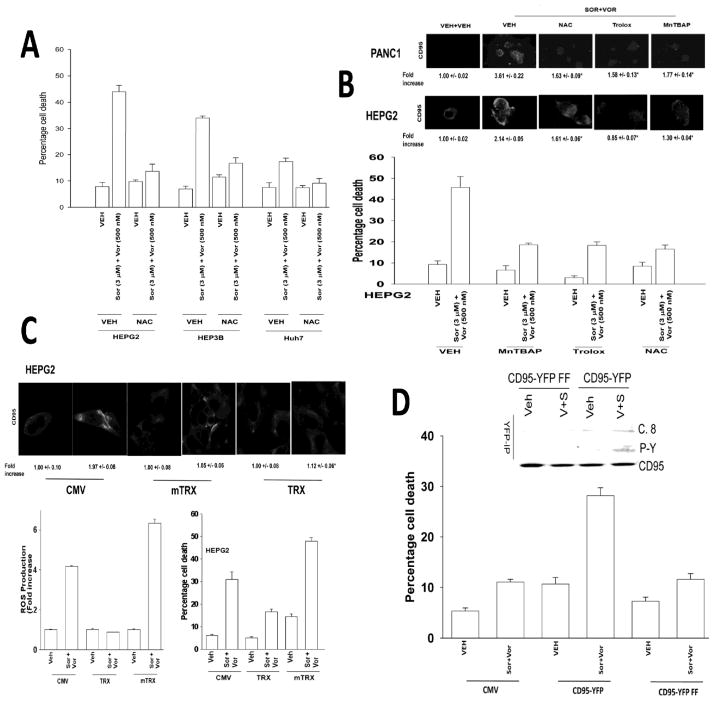
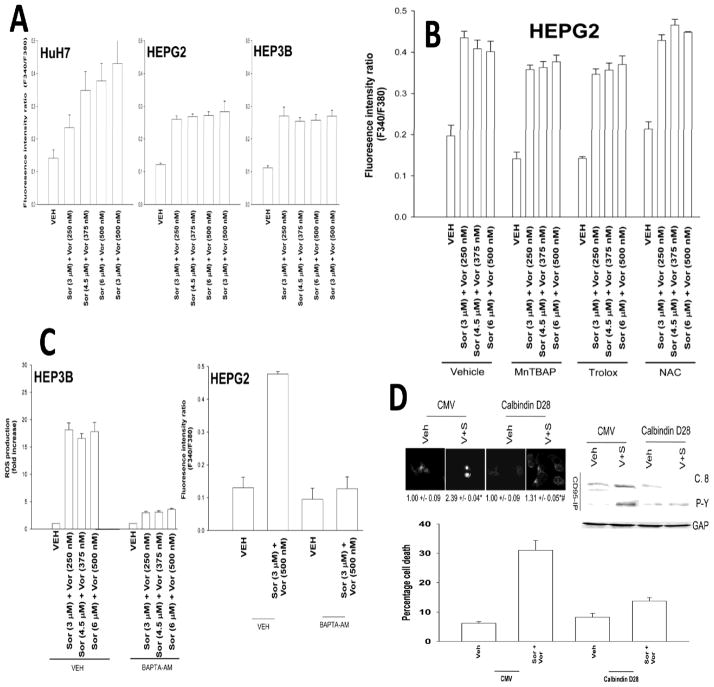
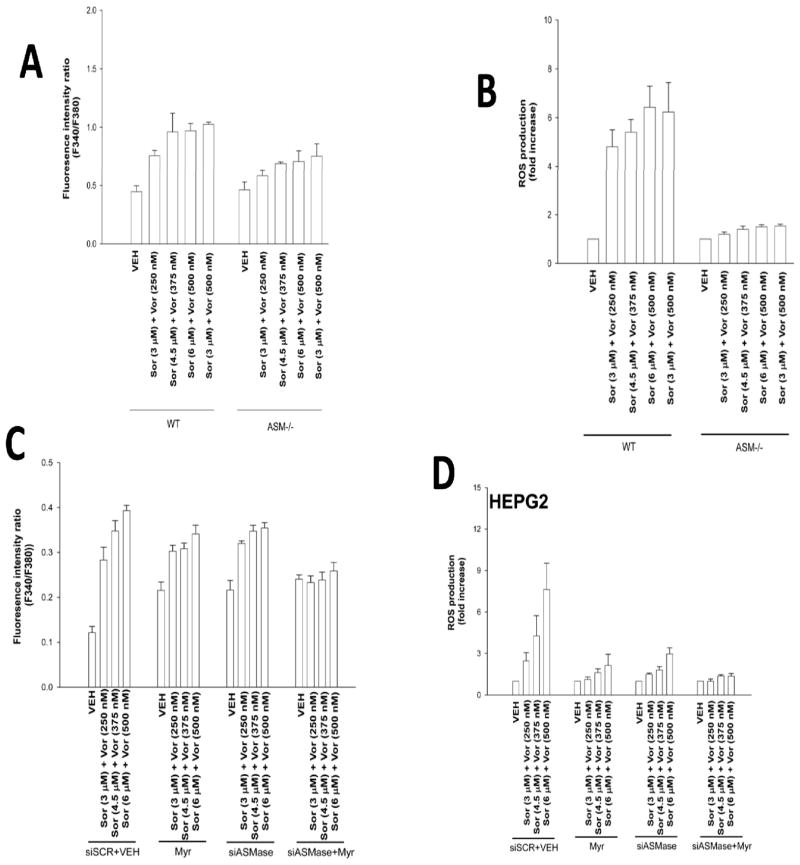
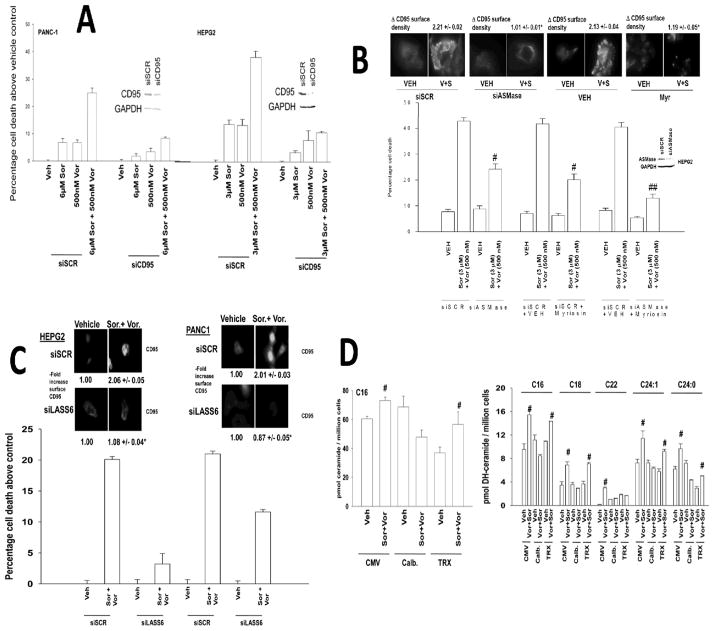
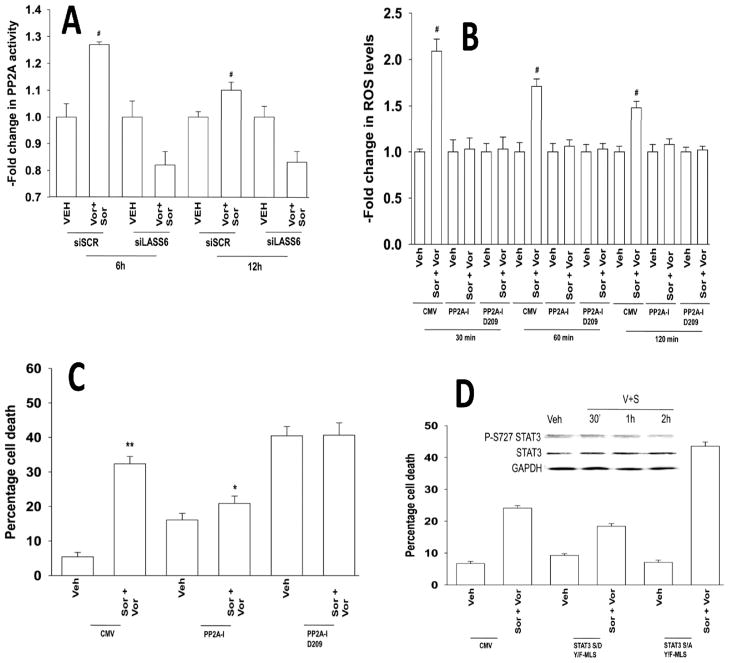
The targeted therapeutics sorafenib and vorinostat interact in a synergistic fashion to kill carcinoma cells by activating CD95, and this drug combination is entering phase I evaluation. In this study, we determined how CD95 is activated by treatment with this drug combination. Low doses of sorafenib and vorinostat, but not the individual drugs, rapidly increased reactive oxygen species (ROS), Ca(2+), and ceramide levels in gastrointestinal tumor cells. The production of ROS was reduced in Rho zero cells. Quenching ROS blocked drug-induced CD95 surface localization and apoptosis. ROS generation, CD95 activation, and cell killing was also blocked by quenching of induced Ca(2+) levels or by inhibition of PP2A. Inhibition of acidic sphingomyelinase or de novo ceramide generation blocked the induction of ROS; however, combined inhibition of both acidic sphingomyelinase and de novo ceramide generation was required to block the induction of Ca(2+). Quenching of ROS did not affect drug-induced ceramide/dihydro-ceramide levels, whereas quenching of Ca(2+) reduced the ceramide increase. Sorafenib and vorinostat treatment radiosensitized liver and pancreatic cancer cells, an effect that was suppressed by quenching ROS or knockdown of LASS6. Further, sorafenib and vorinostat treatment suppressed the growth of pancreatic tumors in vivo. Our findings show that induction of cytosolic Ca(2+) by sorafenib and vorinostat is a primary event that elevates dihydroceramide levels, each essential steps in ROS generation that promotes CD95 activation.
Figures
References
-
- Parkin DM, Bray F, Ferlay J, Pisani P. Global cancer statistics, 2002. CA Cancer J Clin. 2005;55:74–108. - PubMed
-
- Bilimoria KY, Bentrem DJ, Lillemoe KD, Talamonti MS, Ko CY Pancreatic Cancer Quality Indicator Development Expert Panel, American College of Surgeons. Assessment of pancreatic cancer care in the United States based on formally developed quality indicators. J Natl Cancer Inst. 2009;101:848–59. - PMC - PubMed
-
- Dent P. MAP kinase pathways in the control of hepatocyte growth, metabolism and survival. In: Dufour JF, Clavien P-A, editors. Signaling Pathways in Liver Diseases. Chapter 19. Springer Press; 2005. pp. 223–238.
-
- Dent P, Yacoub A, Fisher PB, Hagan MP, Grant S. MAPK pathways in radiation responses. Oncogene. 2003;22:5885–96. - PubMed
-
- Valerie K, Yacoub A, Hagan MP, et al. Radiation-induced cell signaling: inside-out and outside-in. Mol Cancer Ther. 2007;6:789–801. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
