

Sessile serrated adenomas: demographic, endoscopic and pathological characteristics
- PMID: 20632442
- PMCID: PMC2904886
- DOI: 10.3748/wjg.v16.i27.3402
Sessile serrated adenomas: demographic, endoscopic and pathological characteristics
Abstract
Aim: To study the demographic and endoscopic characteristics of patients with sessile serrated adenoma (SSA) in a single center.
Methods: Patients with SSA were identified by review of the pathology database of Mayo Clinic Arizona from 2005 to 2007. A retrospective chart review was performed to extract data on demographics, polyp characteristics, presence of synchronous adenomatous polyps or cancer, polypectomy methods, and related complications.
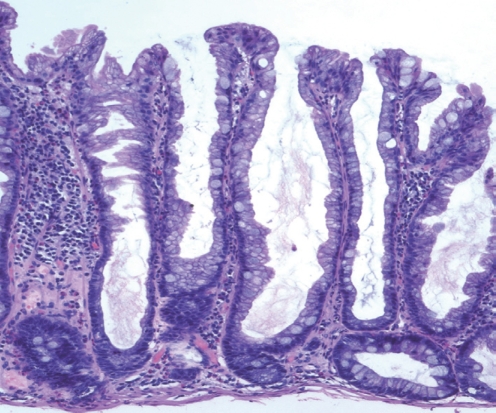
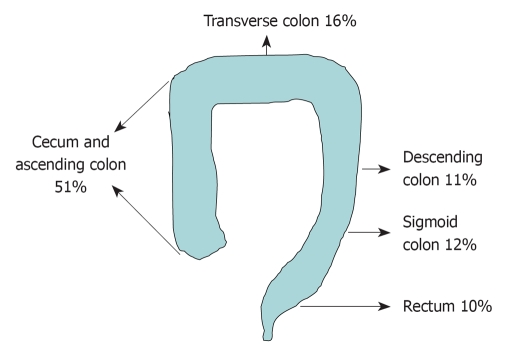
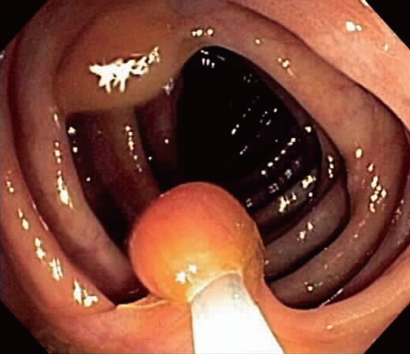
Results: One hundred and seventy-one (2.9%) of all patients undergoing colonoscopy had a total of 226 SSAs. The mean (SE) size of the SSAs was 8.1 (0.4) mm; 42% of SSAs were < or = 5 mm, and 69% were < or = 9 mm. Fifty-one per cent of SSAs were located in the cecum or ascending colon. Approximately half of the patients had synchronous polyps of other histological types, including hyperplastic and adenomatous polyps. Synchronous adenocarcinoma was present in seven (4%) cases. Ninety-seven percent of polyps were removed by colonoscopy.
Conclusion: Among patients with colon polyps, 2.9% were found to have SSAs. Most of the SSAs were located in the right side and were safely managed by colonoscopy.
Figures
Similar articles
-
Outcomes of a 5-year follow-up of patients with sessile serrated adenomas.Scand J Gastroenterol. 2012 Feb;47(2):178-83. doi: 10.3109/00365521.2011.645499. Epub 2012 Jan 10. Scand J Gastroenterol. 2012. PMID: 22229626
-
Variation in the detection of serrated polyps in an average risk colorectal cancer screening cohort.Am J Gastroenterol. 2010 Dec;105(12):2656-64. doi: 10.1038/ajg.2010.315. Epub 2010 Aug 17. Am J Gastroenterol. 2010. PMID: 20717107
-
Optical biopsy of sessile serrated adenomas: do these lesions resemble hyperplastic polyps under narrow-band imaging?Gastrointest Endosc. 2013 Dec;78(6):902-909. doi: 10.1016/j.gie.2013.06.004. Epub 2013 Jul 9. Gastrointest Endosc. 2013. PMID: 23849819 Free PMC article.
-
Endoscopic diagnosis of sessile serrated adenoma/polyp with and without dysplasia/carcinoma.World J Gastroenterol. 2018 Aug 7;24(29):3250-3259. doi: 10.3748/wjg.v24.i29.3250. World J Gastroenterol. 2018. PMID: 30090005 Free PMC article. Review.
-
Serrated polyps - a concealed but prevalent precursor of colorectal cancer.Scand J Gastroenterol. 2017 Jun-Jul;52(6-7):654-661. doi: 10.1080/00365521.2017.1298154. Epub 2017 Mar 9. Scand J Gastroenterol. 2017. PMID: 28277895 Review.
Cited by
-
Usefulness of the Japan narrow-band imaging expert team classification system for the diagnosis of sessile serrated lesion with dysplasia/carcinoma.Surg Endosc. 2021 Aug;35(8):4528-4538. doi: 10.1007/s00464-020-07967-w. Epub 2020 Sep 9. Surg Endosc. 2021. PMID: 32909209
-
The effect of polyp location and patient gender on the presence of dysplasia in colonic polyps.Clin Transl Gastroenterol. 2012 Jul 26;3(7):e20. doi: 10.1038/ctg.2012.14. Clin Transl Gastroenterol. 2012. PMID: 23238292 Free PMC article.
-
Prevalence and Clinical Features of Sessile Serrated Polyps: A Systematic Review.Gastroenterology. 2020 Jul;159(1):105-118.e25. doi: 10.1053/j.gastro.2020.03.025. Epub 2020 Mar 18. Gastroenterology. 2020. PMID: 32199884 Free PMC article.
-
Serrated polyps of the large intestine: current understanding of diagnosis, pathogenesis, and clinical management.J Gastroenterol. 2013 Mar;48(3):287-302. doi: 10.1007/s00535-012-0720-y. Epub 2012 Dec 4. J Gastroenterol. 2013. PMID: 23208018 Free PMC article. Review.
-
Colonic polyp histopathology and location in a community-based sample of older adults.BMC Gastroenterol. 2016 Aug 2;16(1):90. doi: 10.1186/s12876-016-0497-1. BMC Gastroenterol. 2016. PMID: 27485715 Free PMC article.
References
-
- Vogelstein B, Fearon ER, Hamilton SR, Kern SE, Preisinger AC, Leppert M, Nakamura Y, White R, Smits AM, Bos JL. Genetic alterations during colorectal-tumor development. N Engl J Med. 1988;319:525–532. - PubMed
-
- Goldstein NS, Bhanot P, Odish E, Hunter S. Hyperplastic-like colon polyps that preceded microsatellite-unstable adenocarcinomas. Am J Clin Pathol. 2003;119:778–796. - PubMed
-
- Lindor NM, Burgart LJ, Leontovich O, Goldberg RM, Cunningham JM, Sargent DJ, Walsh-Vockley C, Petersen GM, Walsh MD, Leggett BA, et al. Immunohistochemistry versus microsatellite instability testing in phenotyping colorectal tumors. J Clin Oncol. 2002;20:1043–1048. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
