

Lopinavir tablet pharmacokinetics with an increased dose during pregnancy
- PMID: 20632458
- PMCID: PMC3265163
- DOI: 10.1097/qai.0b013e3181d6c9ed
Lopinavir tablet pharmacokinetics with an increased dose during pregnancy
Abstract
Objective: Reduced lopinavir concentrations have been demonstrated with use of the capsule formulation during the third trimester of pregnancy. This study determined lopinavir exposure with an increased dose of the new tablet formulation during the third trimester.
Design: International Maternal Pediatric Adolescent AIDS Clinical Trials 1026s is a prospective nonblinded pharmacokinetic study in HIV-infected pregnant women, including a cohort receiving 2 lopinavir/ritonavir tablets (400 mg/100 mg) twice daily during the second trimester, 3 tablets (600 mg/150 mg) twice daily during the third trimester, and 2 tablets (400 mg/100 mg) twice daily post delivery through 2 weeks postpartum.
Methods: Steady-state 12-hour pharmacokinetic profiles were performed during pregnancy and at 2 weeks postpartum. Lopinavir and ritonavir were measured by reverse-phase high-performance liquid chromatography (detection limit, 0.09 mcg/mL).
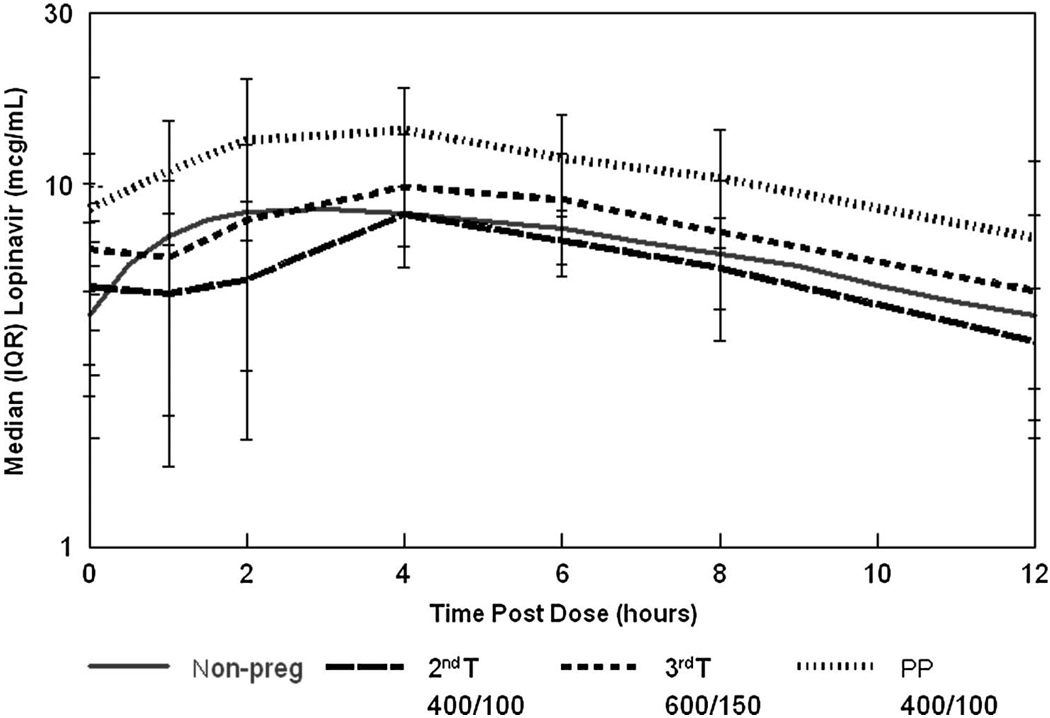
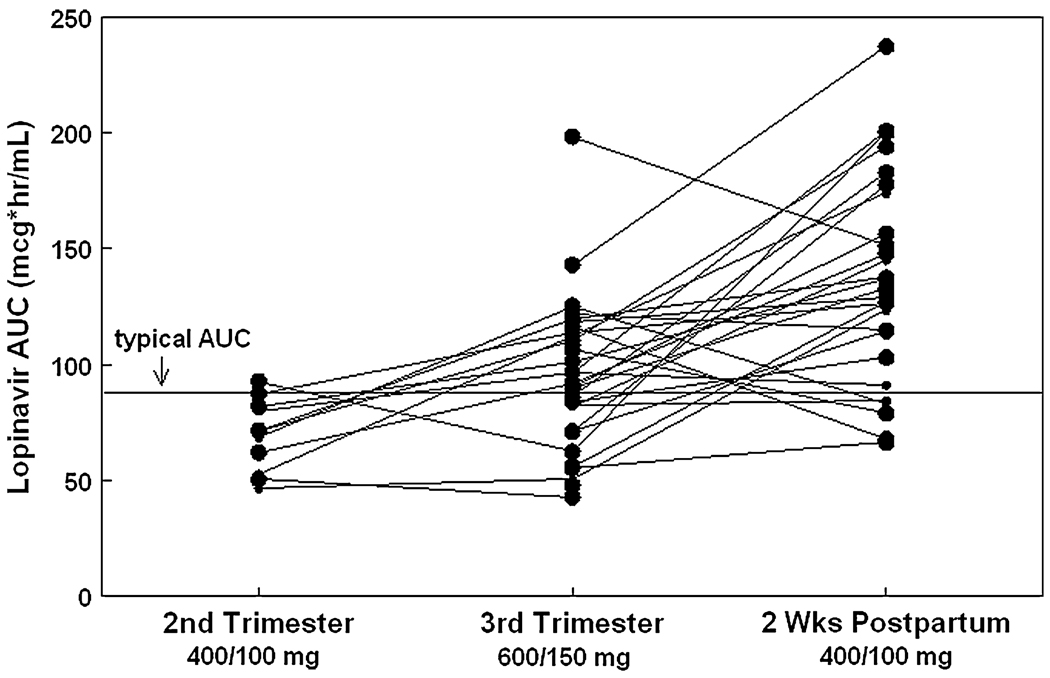
Results: Thirty-three women were studied. Median lopinavir AUC for the second trimester (n = 11), third trimester (n = 33), and postpartum (n = 27) were 72, 96, and 133 mcg x hr/mL, respectively. Median minimum lopinavir concentrations were 3.4, 4.9, and 6.9 mcg/mL.
Conclusions: The higher lopinavir/ritonavir tablet dose (600 mg/150 mg) provided exposure during the third trimester similar to the average AUC (98 mcg x hr x mL(-1) in nonpregnant adults taking 400 mg/100 mg twice daily. The higher dose should be used during the second and third trimesters of pregnancy. Postpartum dosing can be reduced to standard dosing before 2 weeks postpartum.
Figures
References
-
- Shapiro D, Tuomala R, Pollack H, et al. Mother-to-child HIV transmission risk according to antiretroviral therapy, mode of delivery, and viral load in 2895 U.S. women (PACTG 367). Podium presentation at: CROI 2004. Presented at: 11th Conference on Retroviruses and Opportunistic Infections; February 8–11, 2004; San Francisco, CA. Abstract 99.
-
- Perinatal HIV Guidelines Working Group. Public Health Service Task Force Recommendations for Use of Antiretroviral Drugs in Pregnant HIV-Infected Women for Maternal Health and Interventions to Reduce Perinatal HIV Transmission in the United States. Department of Health and Human Services. 2009. Apr 29 [Accessed August 13, 2009]. pp. 1–90. Available at: http://aidsinfo.nih.gov/ContentFiles/PerinatalGL.pdf.
-
- Mirochnick M, Capparelli E. Pharmacokinetics of antiretrovirals in pregnant women. Clin Pharmacokinet. 2004;43:1071–1087. - PubMed
-
- Stek AM, Mirochnick M, Capparelli E, et al. Reduced lopinavir exposure during pregnancy. AIDS. 2006;20:1931–1939. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
