

Microwaves create larger ablations than radiofrequency when controlled for power in ex vivo tissue
- PMID: 20632609
- PMCID: PMC2887908
- DOI: 10.1118/1.3432569
Microwaves create larger ablations than radiofrequency when controlled for power in ex vivo tissue
Abstract
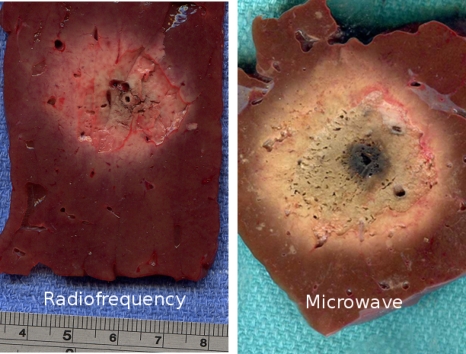
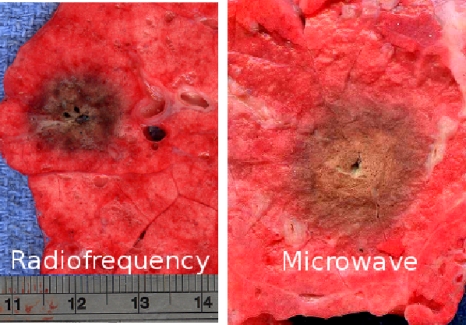
Purpose: To compare ablation zones created with equal amounts of 2.45 GHz microwave and 480 kHz radiofrequency (RF) energy in ex vivo liver and lung.
Methods: A total of 38 ablations were performed in ex vivo liver and lung for 10 min each. Nineteen RF ablations (nine liver, ten lung) were performed with a 480 kHz system (200 W max, impedance-based pulsing) and cooled electrode while measuring the average RF power applied. Nineteen microwave ablations (nine liver, ten lung) were then created using a cooled triaxial antenna to deliver 2.45 GHz at the same power level as in RF experiments. Ablation zones were then sectioned and measured for minimum, maximum and mean diameters, and circularity. Measurements were compared using t-tests, with P < 0.05 indicating statistical significance.
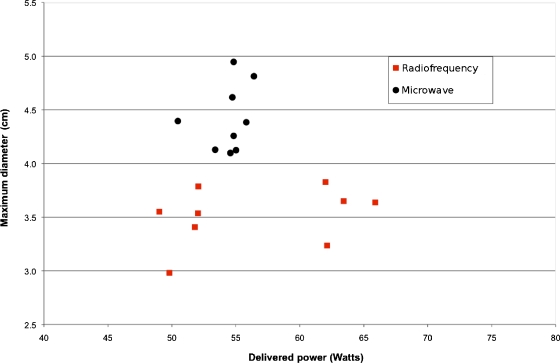
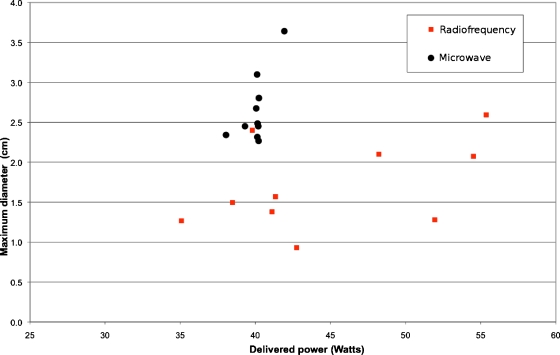
Results: Mean diameters of microwave ablations were greater than RF ablations in both liver and lung (4.4 +/- 0.3 vs 3.3 +/- 0.2 cm in liver; 2.45 +/- 0.3 vs 1.6 +/- 0.5 cm in lungs; P < 0.0005 all comparisons). There was no significant difference in the mean power applied during microwave or RF ablations in either organ (54.44 +/- 1.71 W vs 56.4 +/- 6.7 W in liver, P > 0.05; 40 +/- 0.95 W vs 44.9 +/- 7.1 W in lung, P > 0.05).
Conclusions: Using a single cooled applicator, microwave energy at 2.45 GHz produces larger ablations than an equivalent amount of 480 kHz RF energy in normal liver and lung. This was more apparent in lung, likely due to the high baseline impedance which limits RF, but not microwave power delivery.
Figures
References
-
- Livraghi T., Meloni F., DiStasi M., Rolle E., Solbiati L., Tinelli C., and Rossi S., “Sustained complete response and complications rates after radiofrequency ablation of very early hepatocellular carcinoma in cirrhosis: Is resection still the treatment of choice?,” Hepatology (Baltimore) 47, 82–89 (2008). 10.1002/hep.21933 - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
