

Geographic determinants of reported human Campylobacter infections in Scotland
- PMID: 20633277
- PMCID: PMC2918555
- DOI: 10.1186/1471-2458-10-423
Geographic determinants of reported human Campylobacter infections in Scotland
Abstract
Background: Campylobacteriosis is the leading cause of bacterial gastroenteritis in most developed countries. People are exposed to infection from contaminated food and environmental sources. However, the translation of these exposures into infection in the human population remains incompletely understood. This relationship is further complicated by differences in the presentation of cases, their investigation, identification, and reporting; thus, the actual differences in risk must be considered alongside the artefactual differences.
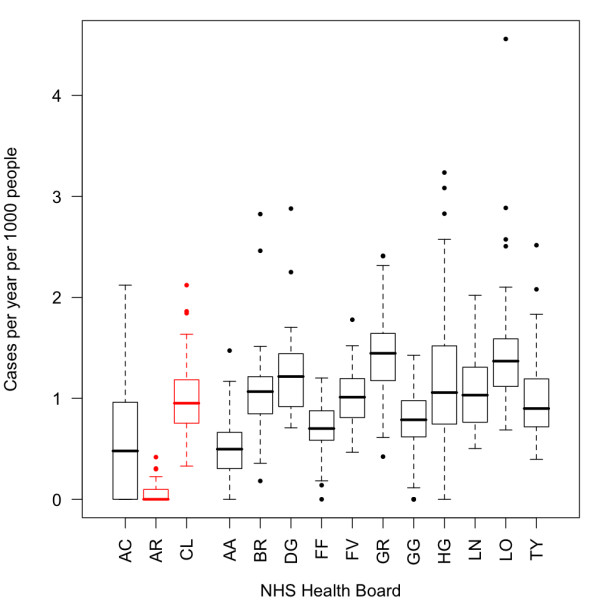
Methods: Data on 33,967 confirmed Campylobacter infections in mainland Scotland between 2000 and 2006 (inclusive) that were spatially referenced to the postcode sector level were analysed. Risk factors including the Carstairs index of social deprivation, the easting and northing of the centroid of the postcode sector, measures of livestock density by species and population density were tested in univariate screening using a non-spatial generalised linear model. The NHS Health Board of the case was included as a random effect in this final model. Subsequently, a spatial generalised linear mixed model (GLMM) was constructed and age-stratified sensitivity analysis was conducted on this model.
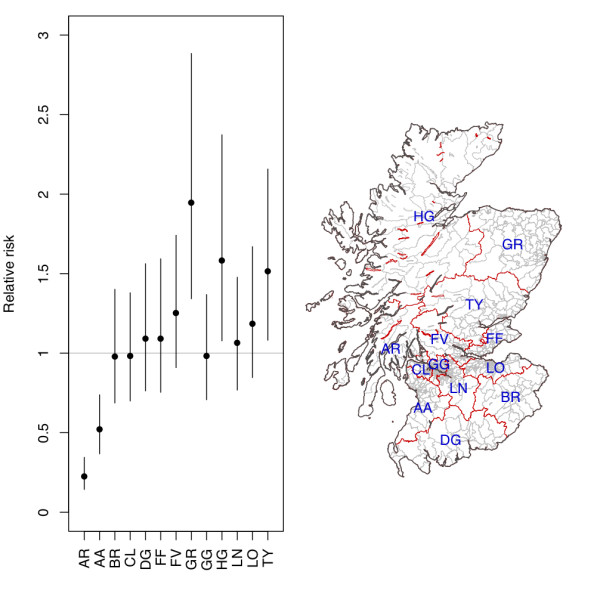
Results: The spatial GLMM included the protective effects of the Carstairs index (relative risk (RR) = 0.965, 95% Confidence intervals (CIs) = 0.959, 0.971) and population density (RR = 0.945, 95% CIs = 0.916, 0.974. Following stratification by age group, population density had a significant protective effect (RR = 0.745, 95% CIs = 0.700, 0.792) for those under 15 but not for those aged 15 and older (RR = 0.982, 95% CIs = 0.951, 1.014). Once these predictors have been taken into account three NHS Health Boards remain at significantly greater risk (Grampian, Highland and Tayside) and two at significantly lower risk (Argyll and Ayrshire and Arran).
Conclusions: The less deprived and children living in rural areas are at the greatest risk of being reported as a case of Campylobacter infection. However, this analysis cannot differentiate between actual risk and heterogeneities in individual reporting behaviour; nevertheless this paper has demonstrated that it is possible to explain the pattern of reported Campylobacter infections using both social and environmental predictors.
Figures

Similar articles
-
Geographic distribution of vestibular schwannomas in West Scotland between 2000-2015.PLoS One. 2017 May 11;12(5):e0175489. doi: 10.1371/journal.pone.0175489. eCollection 2017. PLoS One. 2017. PMID: 28493872 Free PMC article.
-
A population-based exposure assessment of risk factors associated with gastrointestinal pathogens: a Campylobacter study.Epidemiol Infect. 2013 May;141(5):976-86. doi: 10.1017/S0950268812001641. Epub 2012 Aug 9. Epidemiol Infect. 2013. PMID: 22877359 Free PMC article.
-
High level of gastrointestinal nosocomial infections in the german surveillance system, 2002-2008.Infect Control Hosp Epidemiol. 2010 Dec;31(12):1273-8. doi: 10.1086/657133. Infect Control Hosp Epidemiol. 2010. PMID: 21047180
-
Campylobacter species in animal, food, and environmental sources, and relevant testing programs in Canada.Can J Microbiol. 2015 Oct;61(10):701-21. doi: 10.1139/cjm-2014-0770. Can J Microbiol. 2015. PMID: 26422448 Review.
-
Relevance of Campylobacter to public health--the need for a One Health approach.Int J Med Microbiol. 2014 Oct;304(7):817-23. doi: 10.1016/j.ijmm.2014.08.015. Epub 2014 Aug 30. Int J Med Microbiol. 2014. PMID: 25266744 Review.
Cited by
-
Non food-related risk factors of campylobacteriosis in Canada: a matched case-control study.BMC Public Health. 2016 Sep 27;16(1):1016. doi: 10.1186/s12889-016-3679-4. BMC Public Health. 2016. PMID: 27677338 Free PMC article.
-
Overview of the Use of Probiotics in Poultry Production.Animals (Basel). 2021 May 31;11(6):1620. doi: 10.3390/ani11061620. Animals (Basel). 2021. PMID: 34072694 Free PMC article. Review.
-
Seasonal Variability of Thermophilic Campylobacter Spp. in Raw Milk Sold by Automatic Vending Machines in Lombardy Region.Ital J Food Saf. 2016 Jun 16;5(3):5848. doi: 10.4081/ijfs.2016.5848. eCollection 2016 Jun 3. Ital J Food Saf. 2016. PMID: 27853714 Free PMC article.
-
Food-borne disease and climate change in the United Kingdom.Environ Health. 2017 Dec 5;16(Suppl 1):117. doi: 10.1186/s12940-017-0327-0. Environ Health. 2017. PMID: 29219100 Free PMC article. Review.
-
Socioeconomic status and campylobacteriosis, Connecticut, USA, 1999-2009.Emerg Infect Dis. 2014 Jul;20(7):1240-2. doi: 10.3201/eid2007.131333. Emerg Infect Dis. 2014. PMID: 24964129 Free PMC article. No abstract available.
References
-
- Locking M, Browning L, Smith-Palmer A, Brownlie S. Gastro-intestinal and foodborne infections. HPS Weekly Report. 2007;41:3–4.
-
- Wheeler JG, Sethi D, Cowden JM, Wall PG, Rodrigues LC, Tompkins DS, Hudson MJ, Roderick PJ. Study of infectious intestinal disease in England: rates in the community, presenting to general practice, and reported to national surveillance. The Infectious Intestinal Disease Study Executive. BMJ. 1999;318(7190):1046–1050. - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
