

Preexisting donor-specific HLA antibodies predict outcome in kidney transplantation
- PMID: 20634297
- PMCID: PMC2938596
- DOI: 10.1681/ASN.2009101065
Preexisting donor-specific HLA antibodies predict outcome in kidney transplantation
Abstract
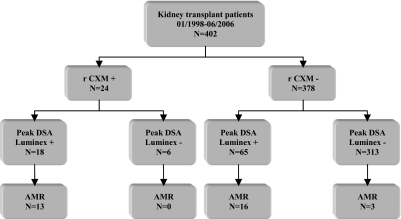
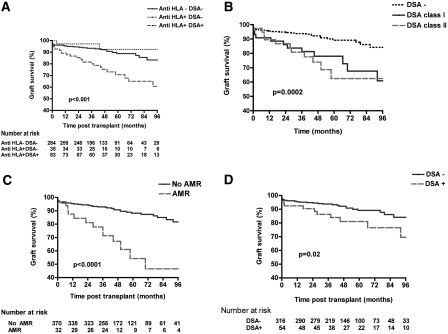
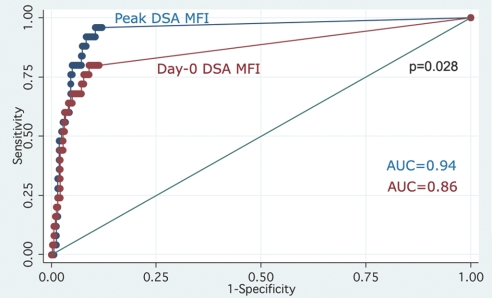
The clinical importance of preexisting HLA antibodies at the time of transplantation, identified by contemporary techniques, is not well understood. We conducted an observational study analyzing the association between preexisting donor-specific HLA antibodies (HLA-DSA) and incidence of acute antibody-mediated rejection (AMR) and survival of patients and grafts among 402 consecutive deceased-donor kidney transplant recipients. We detected HLA-DSA using Luminex single-antigen assays on the peak reactive and current sera. All patients had a negative lymphocytotoxic cross-match test on the day of transplantation. We found that 8-year graft survival was significantly worse (61%) among patients with preexisting HLA-DSA compared with both sensitized patients without HLA-DSA (93%) and nonsensitized patients (84%). Peak HLA-DSA Luminex mean fluorescence intensity (MFI) predicted AMR better than current HLA-DSA MFI (P = 0.028). As MFI of the highest ranked HLA-DSA detected on peak serum increased, graft survival decreased and the relative risk for AMR increased: Patients with MFI >6000 had >100-fold higher risk for AMR than patients with MFI <465 (relative risk 113; 95% confidence interval 31 to 414). The presence of HLA-DSA did not associate with patient survival. In conclusion, the risk for both AMR and graft loss directly correlates with peak HLA-DSA strength. Quantification of HLA antibodies allows stratification of immunologic risk, which should help guide selection of acceptable grafts for sensitized patients.
Figures

References
-
- Organ Procurement and Transplantation Network: Scientific registry of transplant recipients. Available at: http://optn.transplant.hrsa.gov/data/ Accessed May 21, 2010 - PubMed
-
- Cho YW, Cecka J: Crossmatch tests: An analysis of UNOS data from 1991 to 2000. In: Clinical Transplants, edited by Terasaki P, Los Angeles: UCLA Immunogenetics Center, 2001, pp 237–246 - PubMed
-
- Gebel HM, Bray RA, Nickerson P: Pre-transplant assessment of donor-reactive, HLA-specific antibodies in renal transplantation: contraindication vs. risk. Am J Transplant 3: 1488–1500, 2003 - PubMed
-
- Rapport d'activité de prélèvement et de greffe Agence de la Biomédecine. Available at: http://www.agence-biomedecine.fr/uploads/document/RA_1_2_entier.pdf Accessed May 26, 2010
-
- Patel R, Terasaki PI: Significance of the positive crossmatch test in kidney transplantation. N Engl J Med 280: 735–739, 1969 - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
