

Sonographic differentiation of partially cystic thyroid nodules: a prospective study
- PMID: 20634308
- PMCID: PMC7964042
- DOI: 10.3174/ajnr.A2204
Sonographic differentiation of partially cystic thyroid nodules: a prospective study
Abstract
Background and purpose: There is no prospective study related to the sonographic differentiation of malignant PCTN from benign PCTN. This prospective study was designed to evaluate differentiation of benign from malignant PCTNs with thyroid sonography.
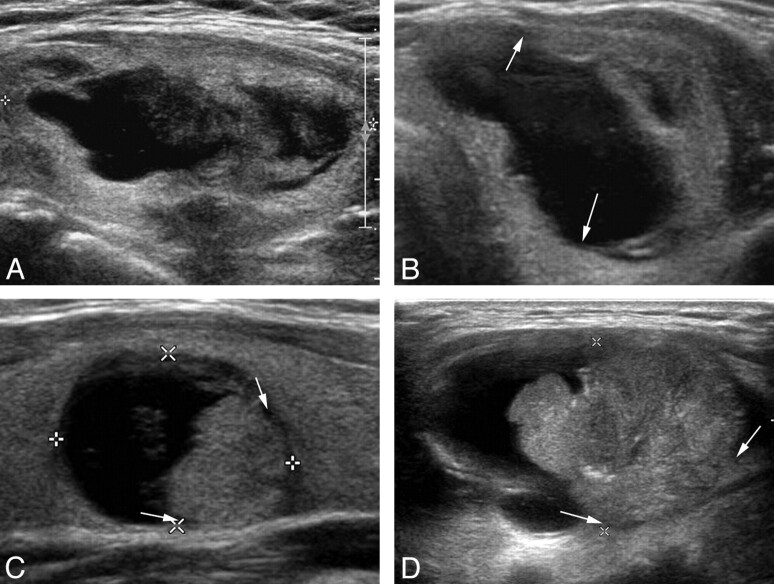
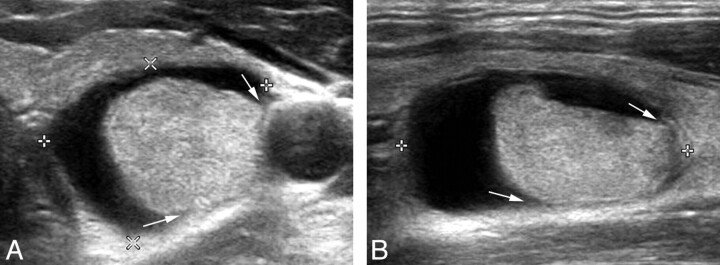
Materials and methods: Two hundred thirteen PCTNs in 196 patients who had consecutively undergone prospective sonographic diagnosis and US-FNAB were included. The PCTNs were evaluated according to their configuration and the presence of calcification, a free margin, vascularity, spongiform appearance or daughter cysts, colloid crystal, nodule shape, and echogenicity. Each PCTN was prospectively classified into 1 of 4 diagnostic categories: benign features, probably benign, suspicious for malignancy, and malignant features. We calculated the diagnostic efficacy of a prospective sonographic diagnosis for PCTNs by comparing it with cytopathologic results.
Results: Among the 213 PCTNs, 53 underwent thyroid surgery. The sonographic classifications for 213 PCTNs included benign features (n = 182), probably benign (n = 19), suspicious for malignancy (n = 7), and malignant features (n = 5). When nonsurgical PCTNs (n = 160) with benign sonographic findings and benign cytology were considered negative, the sensitivity, specificity, PPV, NPV, and accuracy of the prospective diagnosis of PCTNs were 72.7%, 98.0%, 66.7%, 98.5%, and 96.7%, respectively. On the basis of individual analysis, eccentric configuration with an acute angle and microcalcifications were significantly associated with malignancy, but a concentric configuration, a smooth free margin, peripheral vascularity, spongiform appearance or daughter cysts, and intranodular colloid crystals showed a statistically significant association with benignity.
Conclusions: Our prospective sonographic diagnoses of PCTNs, especially those >2 cm, were highly reliable.
Figures
References
-
- McHenry CR, Slusarczyk SJ, Khiyami A. Recommendations for management of cystic thyroid nodule. Surgery 1999;126:1167–72 - PubMed
-
- De Loss Santos ET, Keyhani-Rofagha S, Cunningham JJ, et al. . Cystic thyroid nodules: the dilemma of malignant lesions. Arch Intern Med 1990;150:1422–27 - PubMed
-
- Rosen IB, Provias JB, Walfish PG. Pathologic nature of cystic thyroid nodules selected for surgery by needle aspiration biopsy. Surgery 1986;100:606–12 - PubMed
-
- Bellantone R, Lombardi CP, Raffaelli M, et al. . Management of cystic or predominantly cystic thyroid nodules: the role of ultrasound-guided fine-needle aspiration biopsy. Thyroid 2004;14:43–47 - PubMed
-
- Crile G. Treatment of thyroid cysts by aspiration. Surgery 1966;59:210–12 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical