

Prognostic factors and outcomes of adult patients with acute myeloid leukemia after first relapse
- PMID: 20634493
- PMCID: PMC2966907
- DOI: 10.3324/haematol.2010.027516
Prognostic factors and outcomes of adult patients with acute myeloid leukemia after first relapse
Abstract
Background: Patients with acute myeloid leukemia who are treated with conventional chemotherapy still have a substantial risk of relapse; the prognostic factors and optimal treatments after relapse have not been fully established. We, therefore, retrospectively analyzed data from patients with acute myeloid leukemia who had achieved first complete remission to assess their prognosis after first relapse.
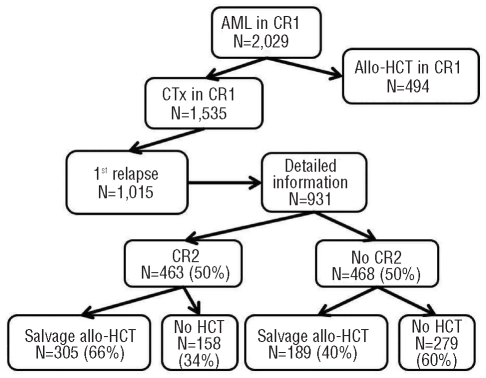
Design and methods: Clinical data were collected from 70 institutions across the country on adult patients who were diagnosed with acute myeloid leukemia and who had achieved a first complete remission after one or two courses of induction chemotherapy.
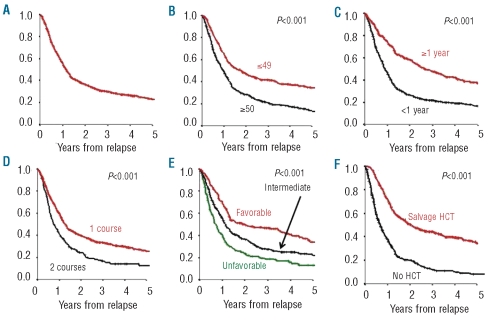
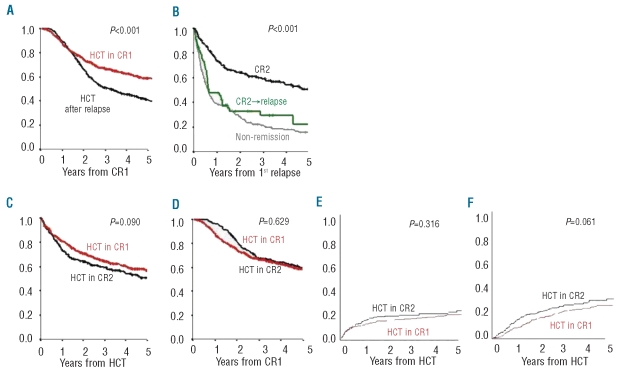
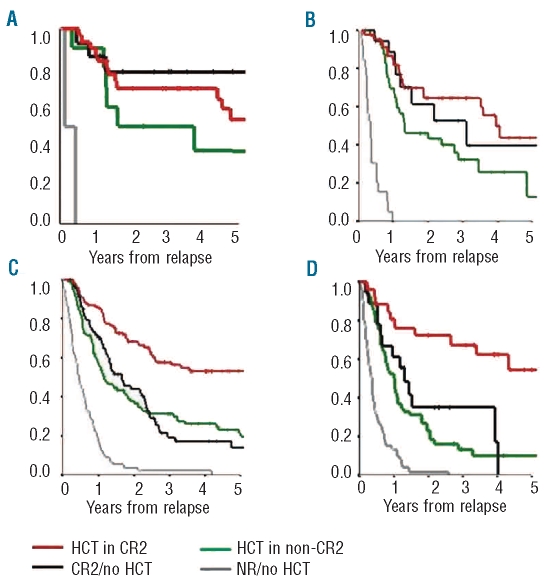
Results: Among the 1,535 patients who were treated with chemotherapy alone, 1,015 relapsed. Half of them subsequently achieved a second complete remission. The overall survival was 30% at 3 years after relapse. Multivariate analysis showed that achievement of second complete remission, salvage allogeneic hematopoietic cell transplantation, and a relapse-free interval of 1 year or longer were independent prognostic factors. The outcome after allogeneic transplantation in second complete remission was comparable to that after transplantation in first complete remission. Patients with acute myeloid leukemia and cytogenetic risk factors other than inv(16) or t(8;21) had a significantly worse outcome when they did not undergo salvage transplantation even when they achieved second complete remission.
Conclusions: We found that both the achievement of second complete remission and the application of salvage transplantation were crucial for improving the prognosis of patients with acute myeloid leukemia in first relapse. Our results indicate that the optimal treatment strategy after first relapse may differ according to the cytogenetic risk.
Figures
Similar articles
-
Monosomal karyotype as an adverse prognostic factor in patients with acute myeloid leukemia treated with allogeneic hematopoietic stem-cell transplantation in first complete remission: a retrospective survey on behalf of the ALWP of the EBMT.Haematologica. 2016 Feb;101(2):248-55. doi: 10.3324/haematol.2015.132654. Epub 2015 Nov 20. Haematologica. 2016. PMID: 26589909 Free PMC article.
-
Core-binding factor acute myeloid leukemia in first relapse: a retrospective study from the French AML Intergroup.Blood. 2014 Aug 21;124(8):1312-9. doi: 10.1182/blood-2014-01-549212. Epub 2014 Jul 8. Blood. 2014. PMID: 25006122 Clinical Trial.
-
Prognosis of patients with core binding factor acute myeloid leukemia after first relapse.Haematologica. 2013 Oct;98(10):1525-31. doi: 10.3324/haematol.2012.078030. Epub 2013 May 28. Haematologica. 2013. PMID: 23716553 Free PMC article.
-
Prognosis of inv(16)/t(16;16) acute myeloid leukemia (AML): a survey of 110 cases from the French AML Intergroup.Blood. 2003 Jul 15;102(2):462-9. doi: 10.1182/blood-2002-11-3527. Epub 2003 Mar 20. Blood. 2003. PMID: 12649129 Review.
-
Relapse and cytogenetic evolution in myeloid neoplasms.Panminerva Med. 2017 Dec;59(4):308-319. doi: 10.23736/S0031-0808.17.03380-8. Panminerva Med. 2017. PMID: 29144072 Review.
Cited by
-
Mitoxantrone and Etoposide for the Treatment of Acute Myeloid Leukemia Patients in First Relapse.Oncol Res. 2016;24(2):73-80. doi: 10.3727/096504016X14586627440156. Oncol Res. 2016. PMID: 27296947 Free PMC article.
-
AML associated oncofusion proteins PML-RARA, AML1-ETO and CBFB-MYH11 target RUNX/ETS-factor binding sites to modulate H3ac levels and drive leukemogenesis.Oncotarget. 2017 Feb 21;8(8):12855-12865. doi: 10.18632/oncotarget.14150. Oncotarget. 2017. PMID: 28030795 Free PMC article.
-
Measurable residual disease status and outcome of transplant in acute myeloid leukemia in second complete remission: a study by the acute leukemia working party of the EBMT.Blood Cancer J. 2021 May 12;11(5):88. doi: 10.1038/s41408-021-00479-3. Blood Cancer J. 2021. PMID: 33980810 Free PMC article.
-
Novel roles of reactive oxygen species in the pathogenesis of acute myeloid leukemia.J Leukoc Biol. 2013 Sep;94(3):423-9. doi: 10.1189/jlb.0113006. Epub 2013 May 28. J Leukoc Biol. 2013. PMID: 23715741 Free PMC article. Review.
-
Treatment of older patients with acute myeloid leukemia (AML): a Canadian consensus.Am J Blood Res. 2013 May 5;3(2):141-64. Print 2013. Am J Blood Res. 2013. PMID: 23675565 Free PMC article.
References
-
- Lowenberg B, Downing JR, Burnett A. Acute myeloid leukemia. N Engl J Med. 1999;341(14):1051–62. - PubMed
-
- Grimwade D, Walker H, Oliver F, Wheatley K, Harrison C, Harrison G, et al. The importance of diagnostic cytogenetics on outcome in AML: analysis of 1,612 patients entered into the MRC AML 10 trial. The Medical Research Council Adult and Children's Leukaemia Working Parties. Blood. 1998;92(7):2322–33. - PubMed
-
- Grimwade D, Hills RK. Independent prognostic factors for AML outcome. Hematology Am Soc Hematol Educ Program. 2009:385–95. - PubMed
-
- Slovak ML, Kopecky KJ, Cassileth PA, Harrington DH, Theil KS, Mohamed A, et al. Karyotypic analysis predicts outcome of preremission and postremission therapy in adult acute myeloid leukemia: a Southwest Oncology Group/Eastern Cooperative Oncology Group study. Blood. 2000;96 (13):4075–83. - PubMed
-
- Leopold LH, Willemze R. The treatment of acute myeloid leukemia in first relapse: a comprehensive review of the literature. Leuk Lymphoma. 2002;43(9):1715–27. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
