

Prediction of cognitive decline in healthy older adults using fMRI
- PMID: 20634590
- PMCID: PMC2940960
- DOI: 10.3233/JAD-2010-091693
Prediction of cognitive decline in healthy older adults using fMRI
Abstract
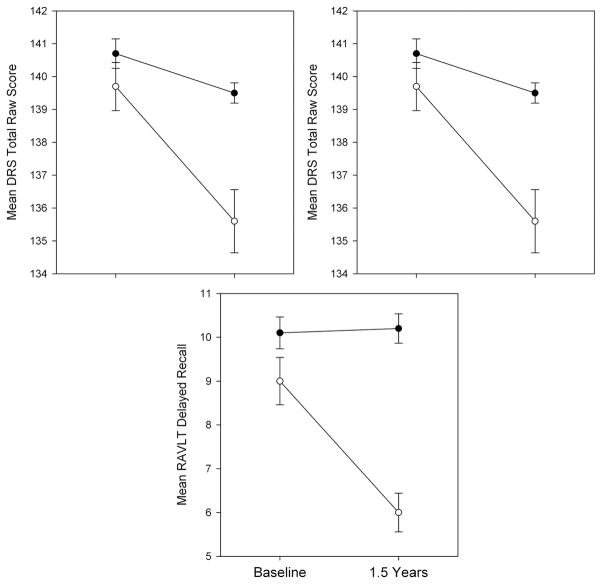
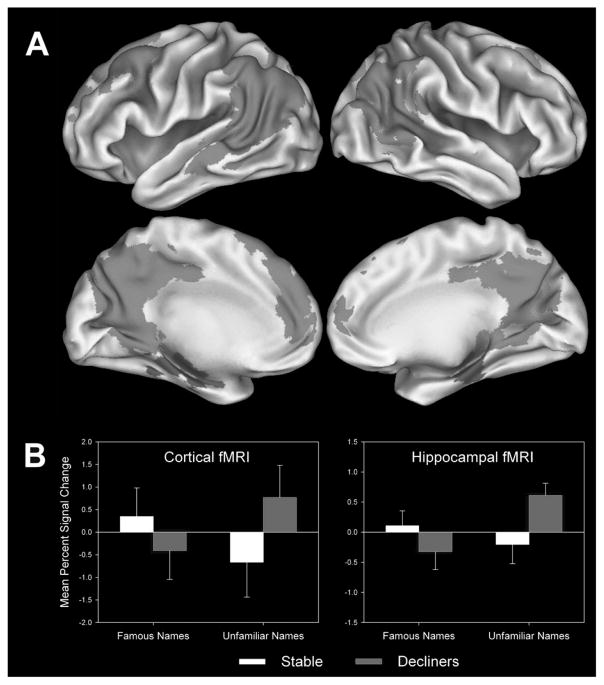
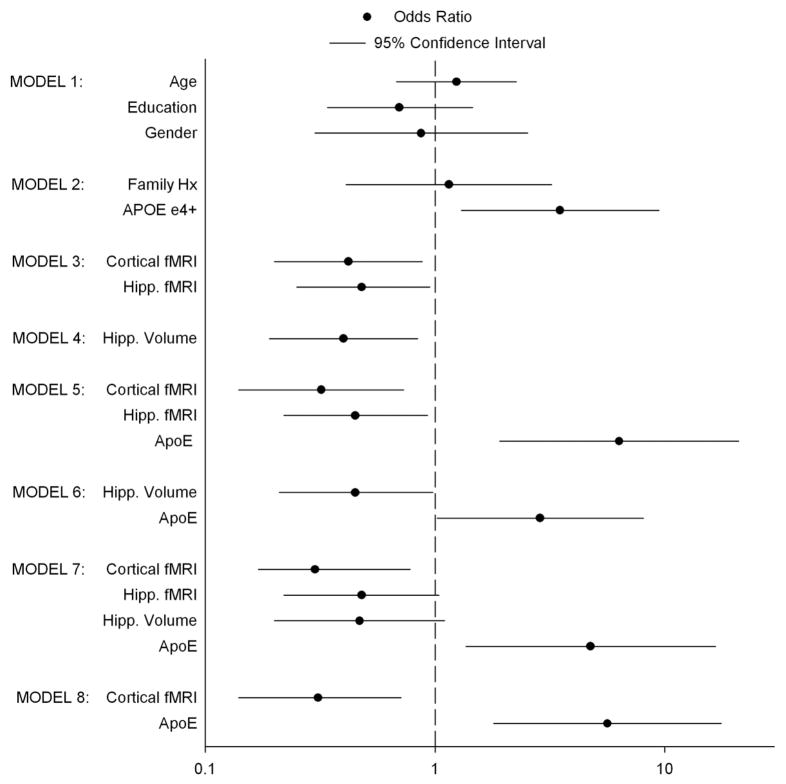
Few studies have examined the extent to which structural and functional MRI, alone and in combination with genetic biomarkers, can predict future cognitive decline in asymptomatic elders. This prospective study evaluated individual and combined contributions of demographic information, genetic risk, hippocampal volume, and fMRI activation for predicting cognitive decline after an 18-month retest interval. Standardized neuropsychological testing, an fMRI semantic memory task (famous name discrimination), and structural MRI (sMRI) were performed on 78 healthy elders (73% female; mean age = 73 years, range = 65 to 88 years). Positive family history of dementia and presence of one or both apolipoprotein E (APOE) ε4 alleles occurred in 51.3% and 33.3% of the sample, respectively. Hippocampal volumes were traced from sMRI scans. At follow-up, all participants underwent a repeat neuropsychological examination. At 18 months, 27 participants (34.6%) declined by at least 1 SD on one of three neuropsychological measures. Using logistic regression, demographic variables (age, years of education, gender) and family history of dementia did not predict future cognitive decline. Greater fMRI activity, absence of an APOE ε4 allele, and larger hippocampal volume were associated with reduced likelihood of cognitive decline. The most effective combination of predictors involved fMRI brain activity and APOE ε4 status. Brain activity measured from task-activated fMRI, in combination with APOE ε4 status, was successful in identifying cognitively intact individuals at greatest risk for developing cognitive decline over a relatively brief time period. These results have implications for enriching prevention clinical trials designed to slow AD progression.
Figures

Similar articles
-
Lifestyle and genetic contributions to cognitive decline and hippocampal structure and function in healthy aging.Curr Alzheimer Res. 2012 May;9(4):436-46. doi: 10.2174/156720512800492477. Curr Alzheimer Res. 2012. PMID: 22272622 Free PMC article.
-
Comparison of semantic and episodic memory BOLD fMRI activation in predicting cognitive decline in older adults.J Int Neuropsychol Soc. 2013 Jan;19(1):11-21. doi: 10.1017/S1355617712000951. Epub 2012 Nov 30. J Int Neuropsychol Soc. 2013. PMID: 23199565 Free PMC article.
-
Semantic memory activation in amnestic mild cognitive impairment.Brain. 2009 Aug;132(Pt 8):2068-78. doi: 10.1093/brain/awp157. Epub 2009 Jun 10. Brain. 2009. PMID: 19515831 Free PMC article.
-
Association between apolipoprotein E ε4 and longitudinal cognitive decline: nested case-control study among chinese community-dwelling elders.Neuropsychobiology. 2011;64(2):102-9. doi: 10.1159/000324991. Epub 2011 Jun 21. Neuropsychobiology. 2011. PMID: 21701228
-
Interactive effects of physical activity and APOE-ε4 on BOLD semantic memory activation in healthy elders.Neuroimage. 2011 Jan 1;54(1):635-44. doi: 10.1016/j.neuroimage.2010.07.070. Epub 2010 Aug 5. Neuroimage. 2011. PMID: 20691792 Free PMC article.
Cited by
-
Do negative affect characteristics and subjective memory concerns increase risk for late life anxiety?J Anxiety Disord. 2013 Aug;27(6):608-18. doi: 10.1016/j.janxdis.2013.03.008. Epub 2013 Apr 3. J Anxiety Disord. 2013. PMID: 23623610 Free PMC article.
-
Lifestyle and genetic contributions to cognitive decline and hippocampal structure and function in healthy aging.Curr Alzheimer Res. 2012 May;9(4):436-46. doi: 10.2174/156720512800492477. Curr Alzheimer Res. 2012. PMID: 22272622 Free PMC article.
-
Vascular and haemodynamic issues of brain ageing.Pflugers Arch. 2021 May;473(5):735-751. doi: 10.1007/s00424-020-02508-9. Epub 2021 Jan 13. Pflugers Arch. 2021. PMID: 33439324 Free PMC article. Review.
-
Loss of Coherence of Low Frequency Fluctuations of BOLD FMRI in Visual Cortex of Healthy Aged Subjects.Open Neuroimag J. 2011;5:105-11. doi: 10.2174/1874440001105010105. Epub 2011 Nov 4. Open Neuroimag J. 2011. PMID: 22216081 Free PMC article.
-
Neuroplastic effects of combined computerized physical and cognitive training in elderly individuals at risk for dementia: an eLORETA controlled study on resting states.Neural Plast. 2015;2015:172192. doi: 10.1155/2015/172192. Epub 2015 Apr 7. Neural Plast. 2015. PMID: 25945260 Free PMC article. Clinical Trial.
References
-
- Kok E, Haikonen S, Luoto T, Huhtala H, Goebeler S, Haapasalo H, Karhunen PJ. Apolipoprotein E-dependent accumulation of Alzheimer disease-related lesions begins in middle age. Ann Neurol. 2009;65:650–657. - PubMed
-
- Albert MS, Moss MB, Tanzi R, Jones K. Preclinical prediction of AD using neuropsychological tests. J Int Neuropsychol Soc. 2001;7:631–639. - PubMed
-
- De Jager CA, Hogervorst E, Combrinck M, Budge MM. Sensitivity and specificity of neuropsychological tests for mild cognitive impairment, vascular cognitive impairment and Alzheimer’s disease. Psychol Med. 2003;33:1039–1050. - PubMed
-
- Nestor PJ, Scheltens P, Hodges JR. Advances in the early detection of Alzheimer’s disease. Nat Med. 2004;10(Suppl):S34–41. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
