

Measuring depression levels in HIV-infected patients as part of routine clinical care using the nine-item Patient Health Questionnaire (PHQ-9)
- PMID: 20635252
- PMCID: PMC3410748
- DOI: 10.1080/09540120903483034
Measuring depression levels in HIV-infected patients as part of routine clinical care using the nine-item Patient Health Questionnaire (PHQ-9)
Abstract
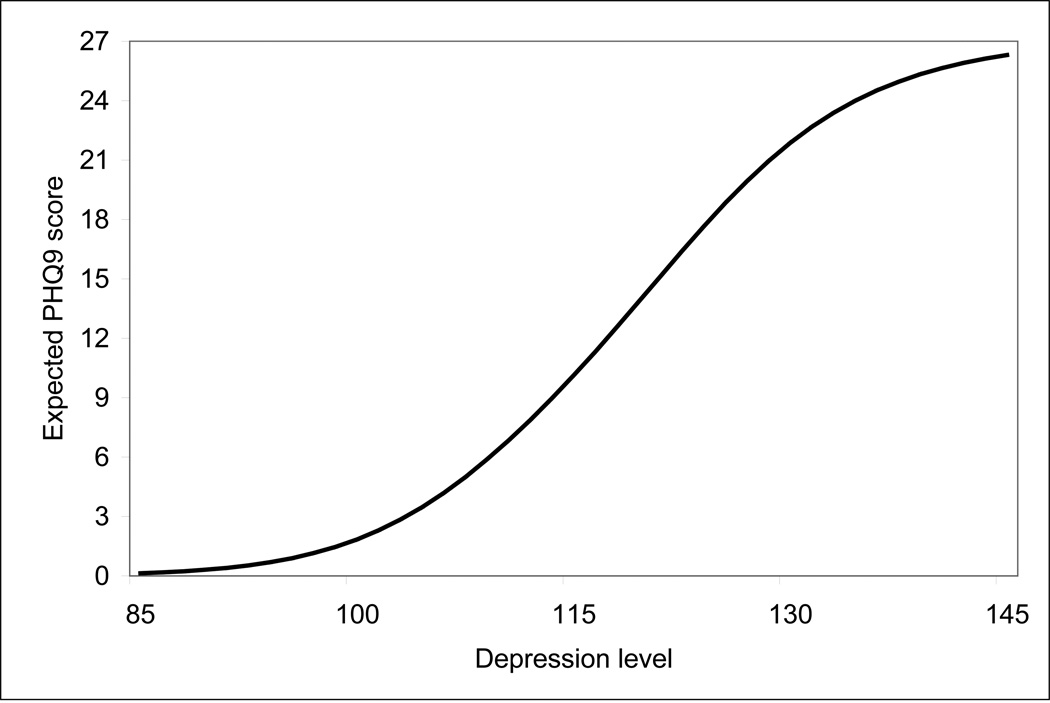
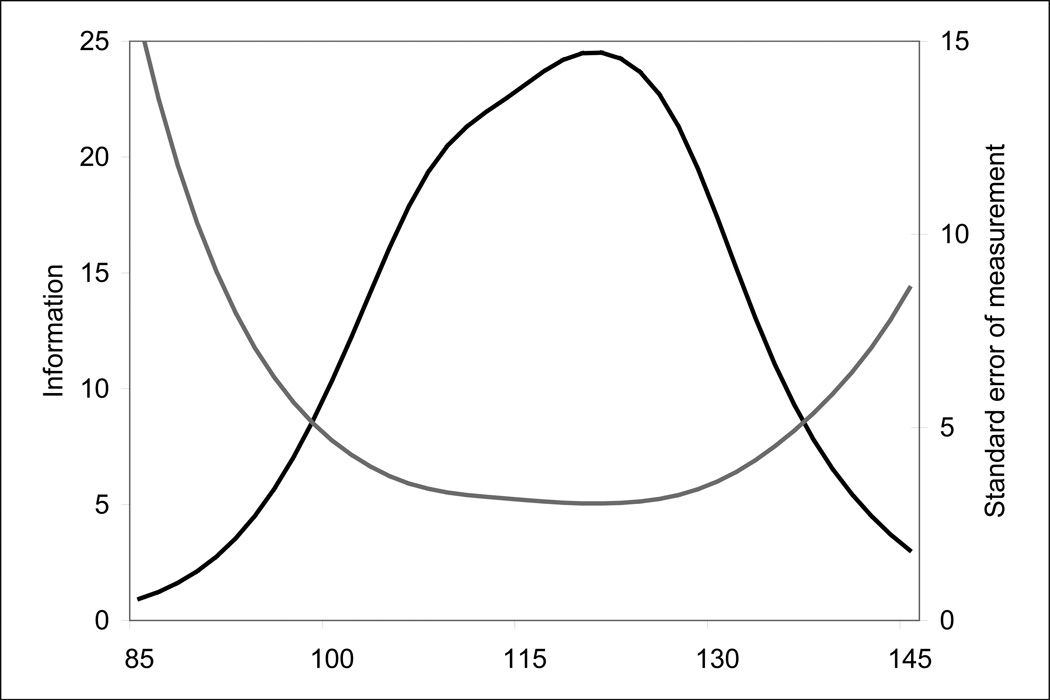
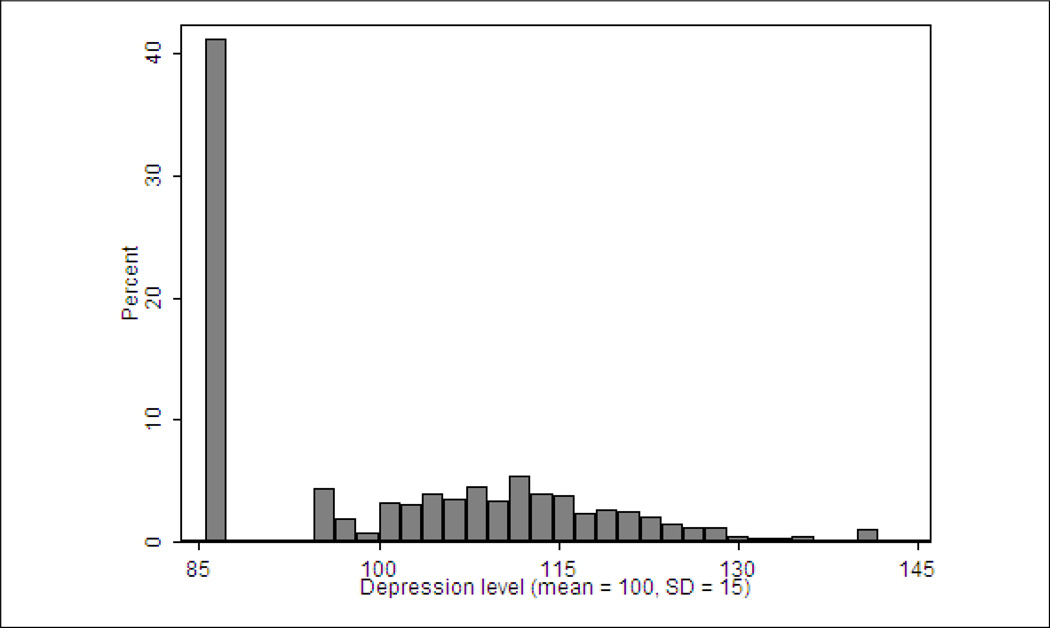
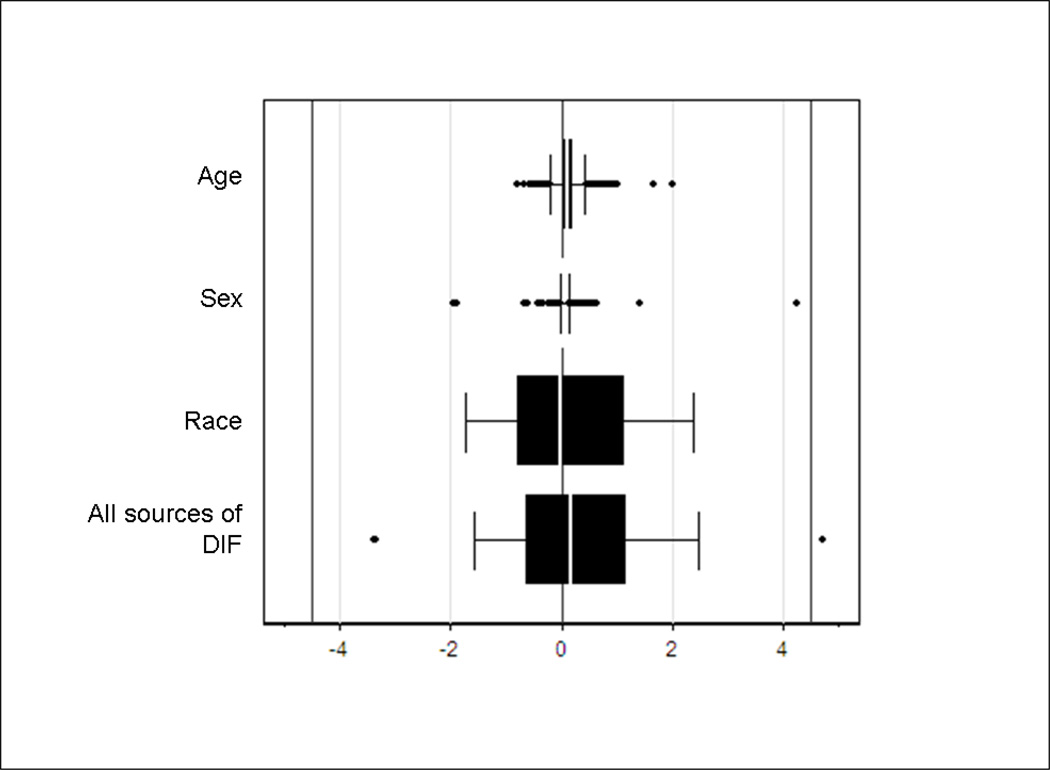
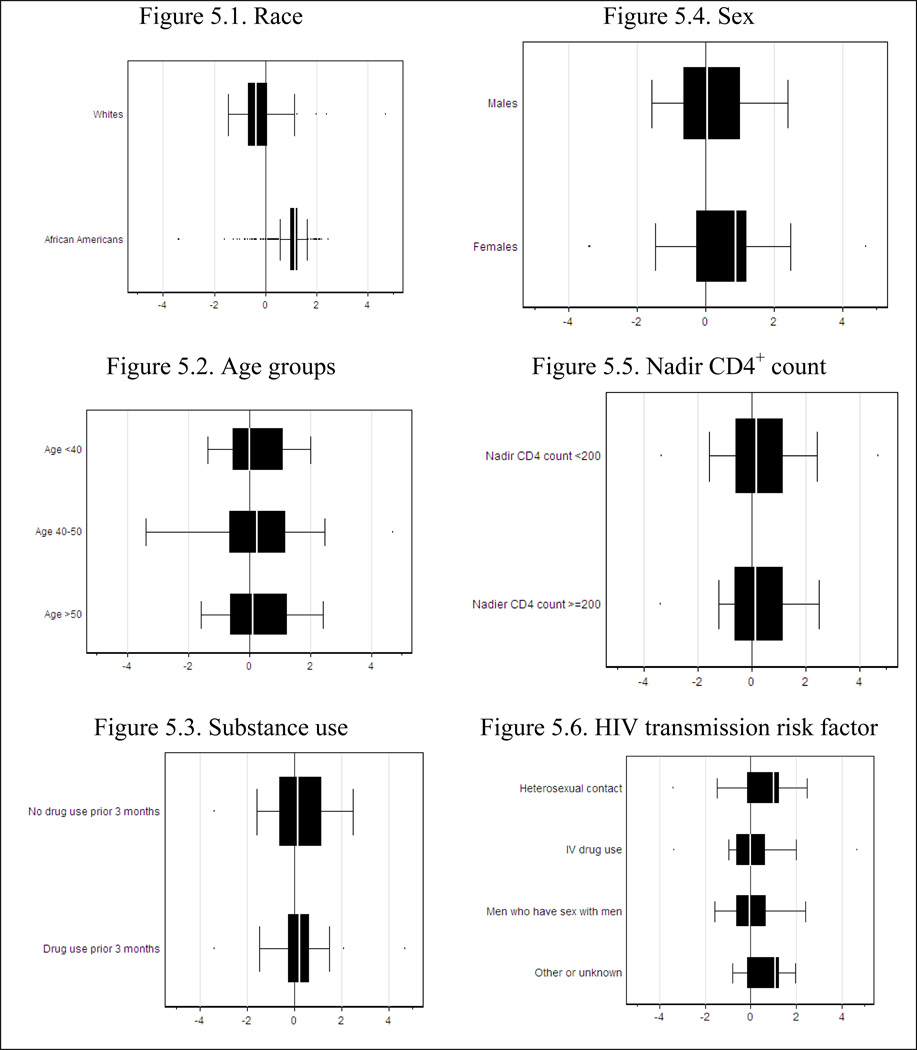
Little is known about the psychometric properties of depression instruments among persons infected with HIV. We analyzed data from a large sample of patients in usual care in two US cities (n=1467) using the nine-item Patient Health Questionnaire (PHQ-9) from the PRIME-MD. The PHQ-9 had curvilinear scaling properties and varying levels of measurement precision along the continuum of depression measured by the instrument. In our cohort, the scale showed a prominent floor effect and a distribution of scores across depression severity levels. Three items had differential item functioning (DIF) with respect to race (African-American vs. white); two had DIF with respect to sex; and one had DIF with respect to age. There was minimal individual-level DIF impact. Twenty percent of the difference in mean depression levels between African-Americans and whites was due to DIF. While standard scores for the PHQ-9 may be appropriate for use with individual HIV-infected patients in cross-sectional settings, these results suggest that investigations of depression across groups and within patients across time may require a more sophisticated analytic framework.
Figures
References
-
- Adewuya AO, Ola BA, Afolabi OO. Validity of the patient health questionnaire (PHQ-9) as a screening tool for depression amongst Nigerian university students. J Affect Disord. 2006;96(1–2):89–93. - PubMed
-
- American Psychiatric Association. Task Force on DSM-IV. Diagnostic and statistical manual of mental disorders : DSM-IV. 4th ed. Washington, DC: American Psychiatric Association; 1994.
-
- Balfour L, Kowal J, Silverman A, Tasca GA, Angel JB, Macpherson PA, et al. A randomized controlled psycho-education intervention trial: Improving psychological readiness for successful HIV medication adherence and reducing depression before initiating HAART. AIDS Care. 2006;18(7):830–838. - PubMed
-
- Blanch J, Rousaud A, Hautzinger M, Martinez E, Peri JM, Andres S, et al. Assessment of the efficacy of a cognitive-behavioural group psychotherapy programme for HIV-infected patients referred to a consultation-liaison psychiatry department. Psychother Psychosom. 2002;71(2):77–84. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical