

Risk factors and predictors for candidemia in pediatric intensive care unit patients: implications for prevention
- PMID: 20636126
- PMCID: PMC3753770
- DOI: 10.1086/655698
Risk factors and predictors for candidemia in pediatric intensive care unit patients: implications for prevention
Abstract
Background: Candida species are the leading cause of invasive fungal infections in hospitalized children and are the third most common isolates recovered from patients with healthcare-associated bloodstream infection in the United States. Few data exist on risk factors for candidemia in pediatric intensive care unit (PICU) patients.
Methods: We conducted a population-based case-control study of PICU patients at Children's Hospital of Philadelphia during the period from 1997 through 2004. Case patients were identified using laboratory records, and control patients were selected from PICU rosters. Control patients were matched to case patients by incidence density sampling, adjusting for time at risk. Following conditional multivariate analysis, we performed weighted multivariate analysis to determine predicted probabilities for candidemia given certain risk factor combinations.
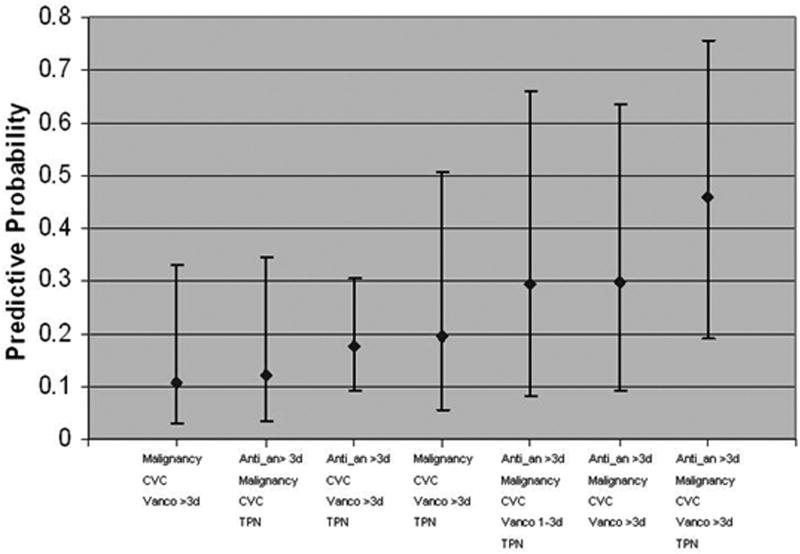
Results: We identified 101 case patients with candidemia (incidence, 3.5 cases per 1000 PICU admissions). Factors independently associated with candidemia included presence of a central venous catheter (odds ratio [OR], 30.4; 95% confidence interval [CI], 7.7-119.5), malignancy (OR, 4.0; 95% CI, 1.23-13.1), use of vancomycin for >3 days in the prior 2 weeks (OR, 6.2; 95% CI, 2.4-16), and receipt of agents with activity against anaerobic organisms for >3 days in the prior 2 weeks (OR, 3.5; 95% CI, 1.5-8.4). Predicted probability of having various combinations of the aforementioned factors ranged from 10.7% to 46%. The 30-day mortality rate was 44% among case patients and 14% among control patients (OR, 4.22; 95% CI, 2.35-7.60).
Conclusions: To our knowledge, this is the first study to evaluate independent risk factors and to determine a population of children in PICUs at high risk for developing candidemia. Future efforts should focus on validation of these risk factors identified in a different PICU population and development of interventions for prevention of candidemia in critically ill children.
Conflict of interest statement
Figures
References
-
- Wisplinghoff H, Seifert H, Tallent SM, Bischoff T, Wenzel RP, Edmond MB. Nosocomial bloodstream infections in pediatric patients in United States hospitals: epidemiology, clinical features and susceptibilities. Pediatr Infect Dis J. 2003 Sep;22(8):686–691. - PubMed
-
- Rex JH, Walsh TJ, Sobel JD, et al. Practice guidelines for the treatment of candidiasis. Infectious Diseases Society of America. Clin Infect Dis. 2000 Apr;30(4):662–678. - PubMed
-
- Martin GS, Mannino DM, Eaton S, Moss M. The epidemiology of sepsis in the United States from 1979 through 2000. N Engl J Med. 2003 Apr 17;348(16):1546–1554. - PubMed
-
- Watson RS, Carcillo JA, Linde-Zwirble WT, Clermont G, Lidicker J, Angus DC. The epidemiology of severe sepsis in children in the United States. Am J Respir Crit Care Med. 2003 Mar 1;167(5):695–701. - PubMed
-
- Zaoutis TE, Argon J, Chu J, Berlin JA, Walsh TJ, Feudtner C. The epidemiology and attributable outcomes of candidemia in adults and children hospitalized in the United States: a propensity analysis. Clin Infect Dis. 2005 Nov 1;41(9):1232–1239. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
