

Female reproductive system and bone
- PMID: 20637179
- PMCID: PMC2942975
- DOI: 10.1016/j.abb.2010.07.006
Female reproductive system and bone
Abstract
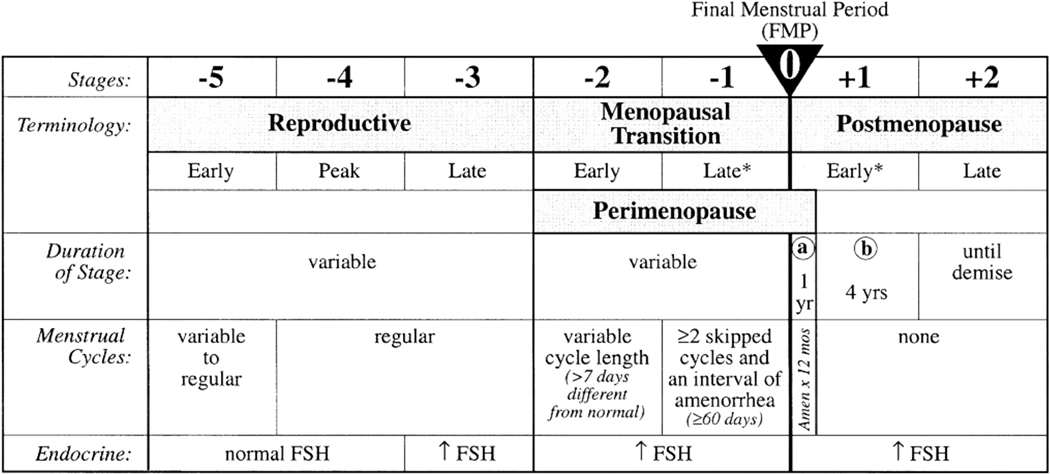
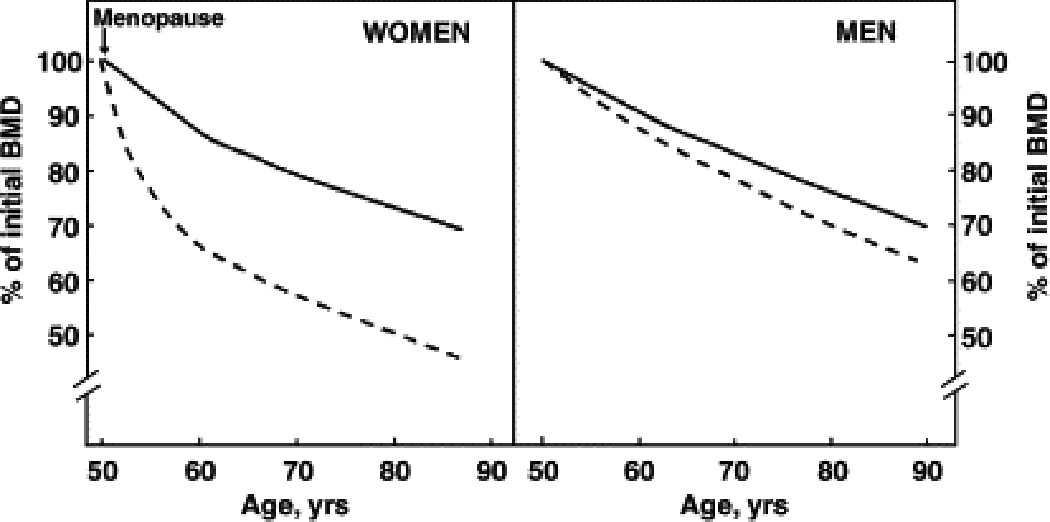
The female reproductive system plays a major role in regulating the acquisition and loss of bone by the skeleton from menarche through senescence. Onset of gonadal sex steroid secretion at puberty is the major factor responsible for skeletal longitudinal and radial growth, as well as significant gain in bone density, until peak bone density is achieved in third decade of life. Gonadal sex steroids then help maintain peak bone density until menopause, including during the transient changes in skeletal mineral content associated with pregnancy and lactation. At menopause, decreased gonadal sex steroid production normally leads to rapid bone loss. The most rapid bone loss associated with decreased estrogen levels occurs in the first 8-10 years after menopause, with slower age-related bone loss occurring during later life. Age-related bone loss in women after the early menopausal phase of bone loss is caused by ongoing gonadal sex steroid deficiency, vitamin D deficiency, and secondary hyperparathyroidism. Other factors also contribute to age-related bone loss, including intrinsic defects in osteoblast function, impairment of the GH/IGF axis, reduced peak bone mass, age-associated sarcopenia, and various sporadic secondary causes. Further understanding of the relative contributions of the female reproductive system and each of the other factors to development and maintenance of the female skeleton, bone loss, and fracture risk will lead to improved approaches for prevention and treatment of osteoporosis.
Copyright © 2010 Elsevier Inc. All rights reserved.
Figures
References
-
- Treloar AE, Boynton RE, Benn BG, et al. Variation in human menstrual cycle through reproductive life. Int. J. Fertil. 1967;12:77–126. - PubMed
-
- Baldwin RM, Whalley PJ, Pritchard JA. Measurements of menstrual blood loss. Am. J. Obstet. Gynecol. 1961;81:739–742. - PubMed
-
- Midgely AR, Jr, Jaffe RB. Regulation of gonadotropins. IV. Correlations of serum concentrations of follicle stimulating and luteinizing hormones during the menstrual cycle. J. Clin. Endocrinol. Metab. 1968;28:1699–1703. - PubMed
-
- Knobil E. The neuroendocrine control of the menstrual cycle. Recent Prog. Horm. Res. 1980;36:53–88. - PubMed
-
- Midgely AR, Jr, Jaffe RB. Regulation of human gonadotropins. X. Episodic fluctuation of LH during the menstrual cycle. J. Clin. Endocrinol. Metab. 1971;33:962–969. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
