

Prognosis of patients with HIV-1 infection starting antiretroviral therapy in sub-Saharan Africa: a collaborative analysis of scale-up programmes
- PMID: 20638120
- PMCID: PMC3138328
- DOI: 10.1016/S0140-6736(10)60666-6
Prognosis of patients with HIV-1 infection starting antiretroviral therapy in sub-Saharan Africa: a collaborative analysis of scale-up programmes
Abstract
Background: Prognostic models have been developed for patients infected with HIV-1 who start combination antiretroviral therapy (ART) in high-income countries, but not for patients in sub-Saharan Africa. We developed two prognostic models to estimate the probability of death in patients starting ART in sub-Saharan Africa.
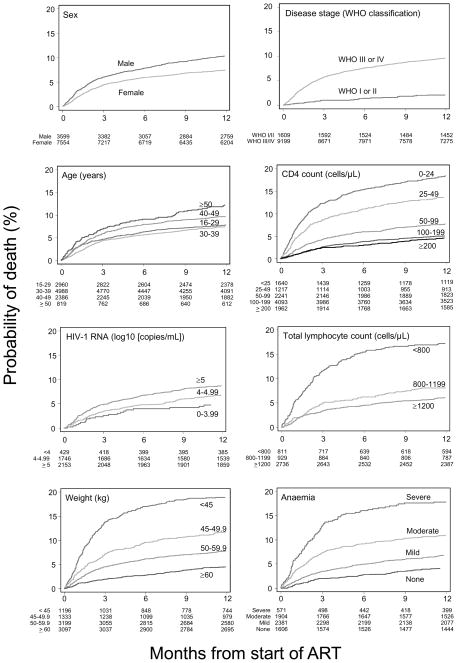
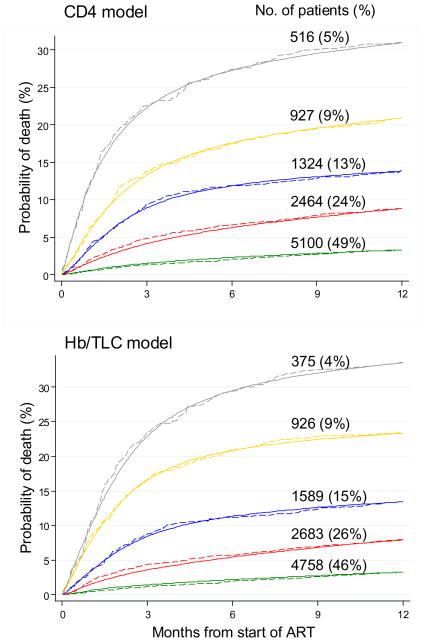
Methods: We analysed data for adult patients who started ART in four scale-up programmes in Côte d'Ivoire, South Africa, and Malawi from 2004 to 2007. Patients lost to follow-up in the first year were excluded. We used Weibull survival models to construct two prognostic models: one with CD4 cell count, clinical stage, bodyweight, age, and sex (CD4 count model); and one that replaced CD4 cell count with total lymphocyte count and severity of anaemia (total lymphocyte and haemoglobin model), because CD4 cell count is not routinely measured in many African ART programmes. Death from all causes in the first year of ART was the primary outcome.
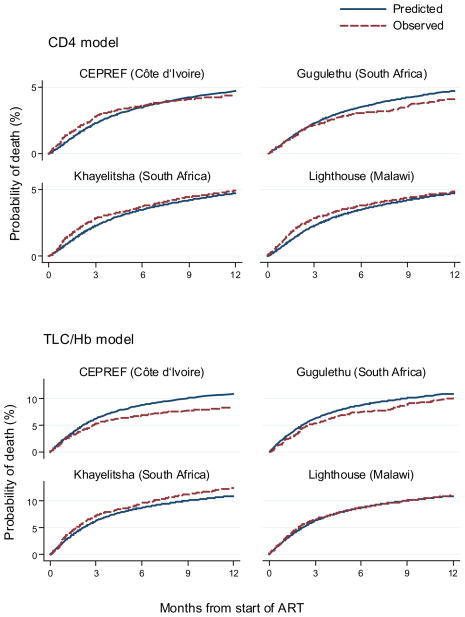
Findings: 912 (8.2%) of 11 153 patients died in the first year of ART. 822 patients were lost to follow-up and not included in the main analysis; 10 331 patients were analysed. Mortality was strongly associated with high baseline CD4 cell count (>/=200 cells per muL vs <25; adjusted hazard ratio 0.21, 95% CI 0.17-0.27), WHO clinical stage (stages III-IV vs I-II; 3.45, 2.43-4.90), bodyweight (>/=60 kg vs <45 kg; 0.23, 0.18-0.30), and anaemia status (none vs severe: 0.27, 0.20-0.36). Other independent risk factors for mortality were low total lymphocyte count, advanced age, and male sex. Probability of death at 1 year ranged from 0.9% (95% CI 0.6-1.4) to 52.5% (43.8-61.7) with the CD4 model, and from 0.9% (0.5-1.4) to 59.6% (48.2-71.4) with the total lymphocyte and haemoglobin model. Both models accurately predict early mortality in patients starting ART in sub-Saharan Africa compared with observed data.
Interpretation: Prognostic models should be used to counsel patients, plan health services, and predict outcomes for patients with HIV-1 infection in sub-Saharan Africa.
Funding: US National Institute of Allergy And Infectious Diseases, Eunice Kennedy Shriver National Institute of Child Health and Human Development, and National Cancer Institute.
Copyright 2010 Elsevier Ltd. All rights reserved.
Conflict of interest statement
We declare that we have no conflict of interest.
Figures
Comment in
-
ART in low-resource settings: how to do more with less.Lancet. 2010 Aug 7;376(9739):396-8. doi: 10.1016/S0140-6736(10)61020-3. Epub 2010 Jul 15. Lancet. 2010. PMID: 20638119 No abstract available.
-
Can we increase male involvement in AIDS treatment?Lancet. 2010 Oct 16;376(9749):1302. doi: 10.1016/S0140-6736(10)61918-6. Lancet. 2010. PMID: 20951892 No abstract available.
References
-
- Egger M, May M, Chene G, Phillips AN, Ledergerber B, Dabis F, et al. Prognosis of HIV-1-infected patients starting highly active antiretroviral therapy: a collaborative analysis of prospective studies. Lancet. 2002;360(9327):119–129. - PubMed
-
- Lundgren JD, Mocroft A, Gatell JM, Ledergerber B, D’Arminio MA, Hermans P, et al. A clinically prognostic scoring system for patients receiving highly active antiretroviral therapy: results from the EuroSIDA study. J Infect Dis. 2002;185(2):178–187. - PubMed
-
- World Health Organization. Towards universal access. Scaling up priority HIV/AIDS interventions in the health sector. Progress Report. 2009 Available from: URL: http://www.who.int/hiv/pub/2009progressreport/en/index.html.
-
- Braitstein P, Brinkhof MW, Dabis F, Schechter M, Boulle A, Miotti P, et al. Mortality of HIV-1-infected patients in the first year of antiretroviral therapy: comparison between low-income and high-income countries. Lancet. 2006;367(9513):817–824. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
