

Vaccine-induced HIV seropositivity/reactivity in noninfected HIV vaccine recipients
- PMID: 20639561
- PMCID: PMC3086635
- DOI: 10.1001/jama.2010.926
Vaccine-induced HIV seropositivity/reactivity in noninfected HIV vaccine recipients
Abstract
Context: Induction of protective anti-human immunodeficiency virus (HIV) immune responses is the goal of an HIV vaccine. However, this may cause a reactive result in routine HIV testing in the absence of HIV infection.
Objective: To evaluate the frequency of vaccine-induced seropositivity/reactivity (VISP) in HIV vaccine trial participants.
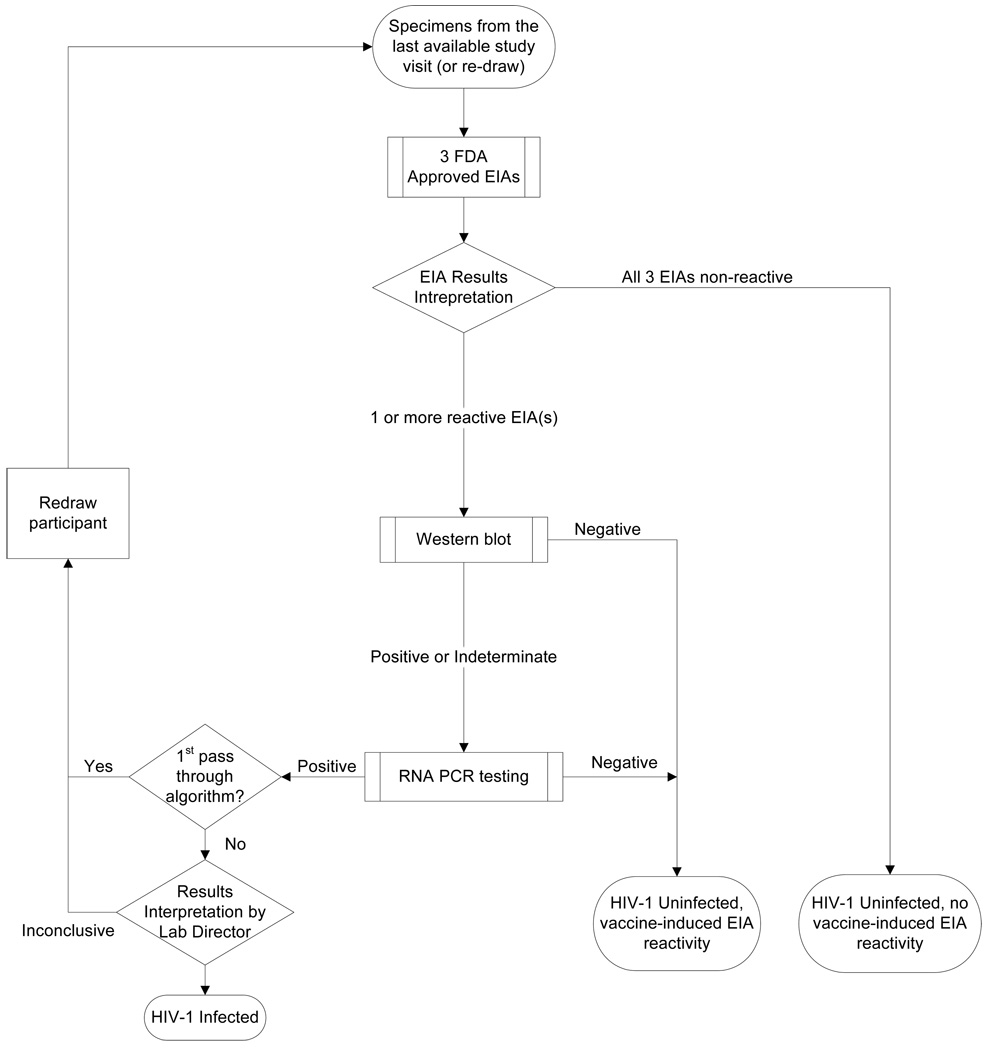
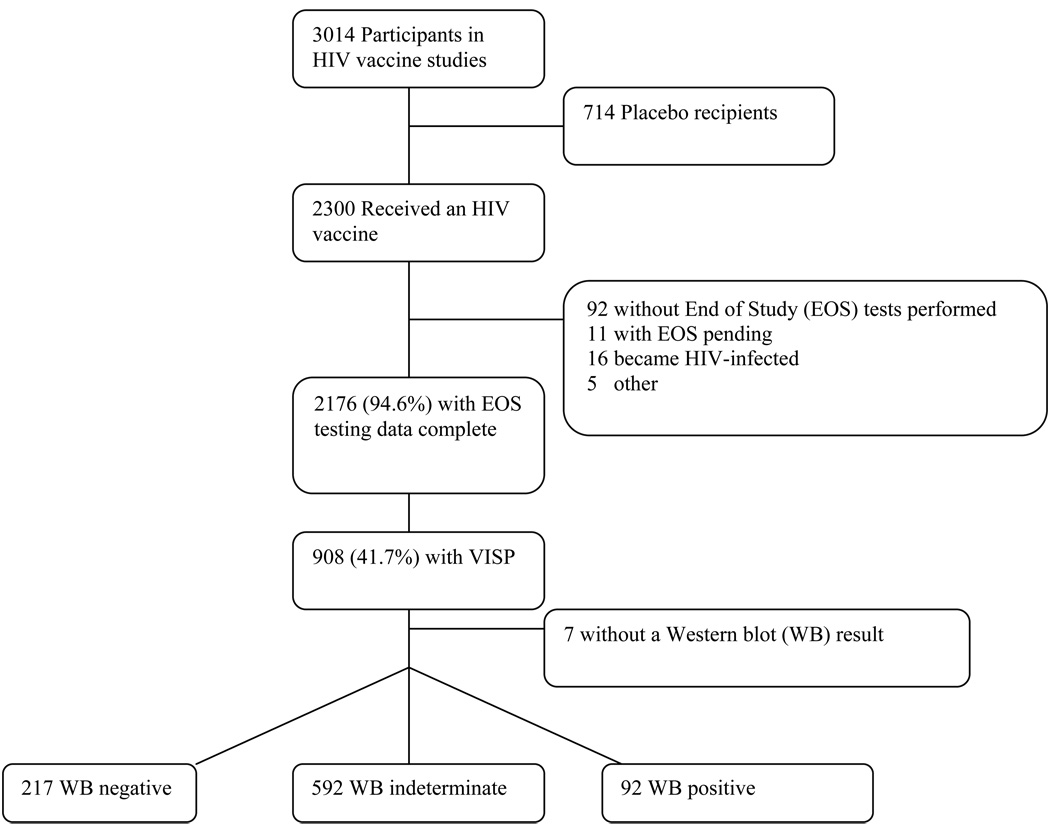
Design, setting, and participants: Three common US Food and Drug Administration-approved enzyme immunoassay (EIA) HIV antibody kits were used to determine VISP, and a routine diagnostic HIV algorithm was used to evaluate VISP frequency in healthy, HIV-seronegative adults who completed phase 1 (n = 25) and phase 2a (n = 2) vaccine trials conducted from 2000-2010 in the United States, South America, Thailand, and Africa.
Main outcome measure: Vaccine-induced seropositivity/reactivity, defined as reactive on 1 or more EIA tests and either Western blot-negative or Western blot-indeterminate/atypical positive (profile consistent with vaccine product) and HIV-1-negative by nucleic acid testing.
Results: Among 2176 participants free of HIV infection who received a vaccine product, 908 (41.7%; 95% confidence interval [CI], 39.6%-43.8%) had VISP, but the occurrence of VISP varied substantially across different HIV vaccine product types: 399 of 460 (86.7%; 95% CI, 83.3%-89.7%) adenovirus 5 product recipients, 295 of 552 (53.4%; 95% CI, 49.2%-57.7%) recipients of poxvirus alone or as a boost, and 35 of 555 (6.3%; 95% CI, 4.4%-8.7%) of DNA-alone product recipients developed VISP. Overall, the highest proportion of VISP (891/2176 tested [40.9%]) occurred with the HIV 1/2 (rDNA) EIA kit compared with the rLAV EIA (150/700 tested [21.4%]), HIV-1 Plus O Microelisa System (193/1309 tested [14.7%]), and HIV 1/2 Peptide and HIV 1/2 Plus O (189/2150 tested [8.8%]) kits. Only 17 of the 908 participants (1.9%) with VISP tested nonreactive using the HIV 1/2 (rDNA) kit. All recipients of a glycoprotein 140 vaccine (n = 70) had VISP, with 94.3% testing reactive with all 3 EIA kits tested. Among 901 participants with VISP and a Western blot result, 92 (10.2%) had a positive Western blot result (displaying an atypical pattern consistent with vaccine product), and 592 (65.7%) had an indeterminate result. Only 8 participants with VISP received a vaccine not containing an envelope insert.
Conclusions: The induction of VISP in HIV vaccine recipients is common, especially with vaccines containing both the HIV-1 envelope and group-specific core antigen gene proteins. Development and detection of VISP appear to be associated with the immunogenicity of the vaccine and the EIA assay used.
Conflict of interest statement
Figures
References
-
- Global Summary of the AIDS epidemic. [Accessed March 15, 2010];2007 December; Available at < http://www.who.int/hiv/data/en/index.html.
-
- Pialoux G, Hocini H, Perusat S, et al. Phase I study of a candidate vaccine based on recombinant HIV-1 gp160 (MN/LAI) administered by the mucosal route to HIV-seronegative volunteers: the ANRS VAC14 study. Vaccine. 2008;26:2657–2666. - PubMed
-
- Pitisuttithum P, Nitayaphan S, Thongcharoen P, et al. Safety and immunogenicity of combinations of recombinant subtype E and B human immunodeficiency virus type 1 envelope glycoprotein 120 vaccines in healthy Thai adults. The Journal of infectious diseases. 2003;188:219–227. - PubMed
-
- Pitisuttithum P, Gilbert P, Gurwith M, et al. Randomized, double-blind, placebo-controlled efficacy trial of a bivalent recombinant glycoprotein 120 HIV-1 vaccine among injection drug users in Bangkok, Thailand. The Journal of infectious diseases. 2006;194:1661–1671. - PubMed
-
- Goepfert PA, Tomaras GD, Horton H, et al. Durable HIV-1 antibody and T-cell responses elicited by an adjuvanted multi-protein recombinant vaccine in uninfected human volunteers. Vaccine. 2007;25:510–518. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- U01 AI069412/AI/NIAID NIH HHS/United States
- AI046703/AI/NIAID NIH HHS/United States
- UM1 AI069412/AI/NIAID NIH HHS/United States
- UM1 AI068618/AI/NIAID NIH HHS/United States
- U01 AI068635/AI/NIAID NIH HHS/United States
- AI068635/AI/NIAID NIH HHS/United States
- AI46725/AI/NIAID NIH HHS/United States
- P30 AI027757/AI/NIAID NIH HHS/United States
- U01 AI046703/AI/NIAID NIH HHS/United States
- UM1 AI068614/AI/NIAID NIH HHS/United States
- U01 AI046725/AI/NIAID NIH HHS/United States
- AI068618/AI/NIAID NIH HHS/United States
- U01 AI046747/AI/NIAID NIH HHS/United States
- UM1 AI068635/AI/NIAID NIH HHS/United States
- AI069412/AI/NIAID NIH HHS/United States
- U01 AI068618/AI/NIAID NIH HHS/United States
- AI068614/AI/NIAID NIH HHS/United States
- U01 AI068614/AI/NIAID NIH HHS/United States
- AI27757/AI/NIAID NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
