

Evaluation of the medicinal use of clay minerals as antibacterial agents
- PMID: 20640226
- PMCID: PMC2904249
- DOI: 10.1080/00206811003679737
Evaluation of the medicinal use of clay minerals as antibacterial agents
Abstract
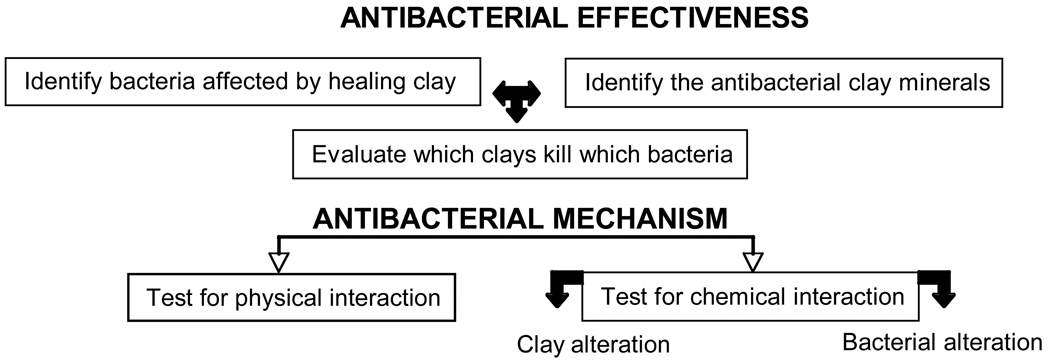
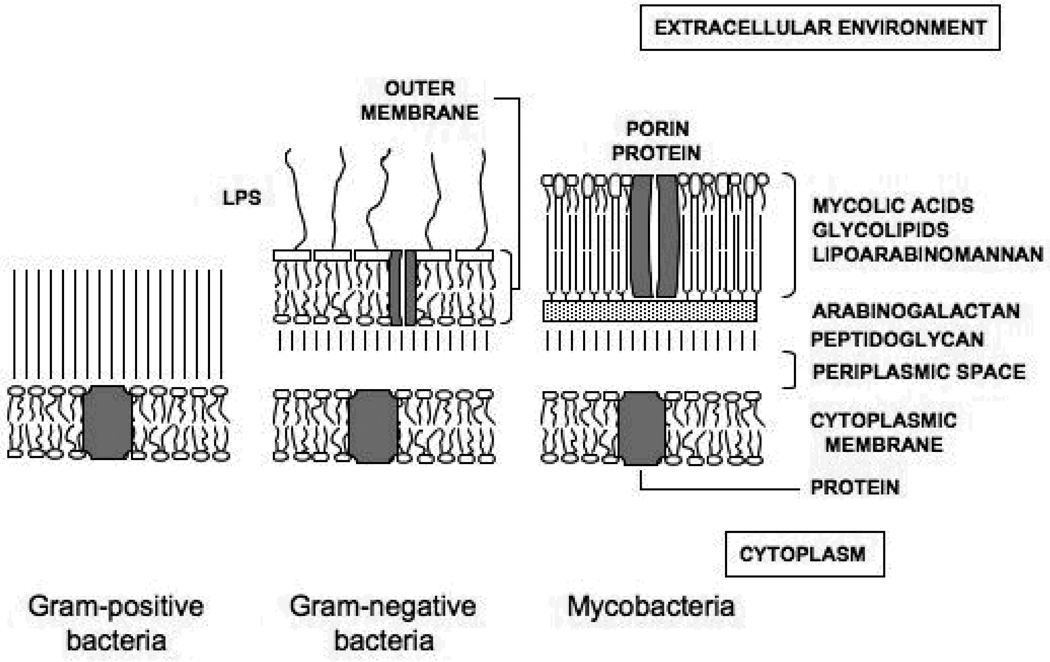
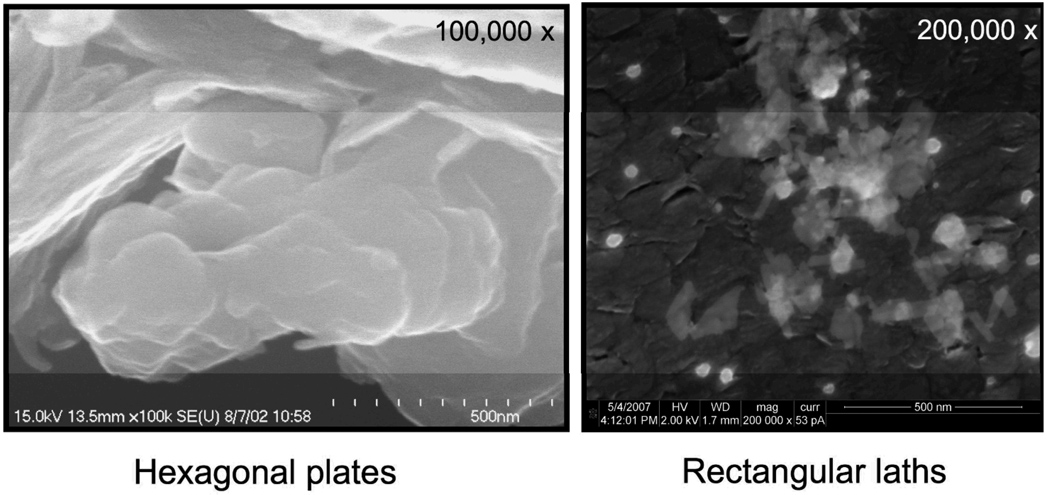
Natural clays have been used to heal skin infections since the earliest recorded history. Recently our attention was drawn to a clinical use of French green clay (rich in Fe-smectite) for healing Buruli ulcer, a necrotizing fasciitis ('flesh-eating' infection) caused by Mycobacterium ulcerans. These clays and others like them are interesting as they may reveal an antibacterial mechanism that could provide an inexpensive treatment for this and other skin infections, especially in global areas with limited hospitals and medical resources.Microbiological testing of two French green clays, and other clays used traditionally for healing, identified three samples that were effective at killing a broad-spectrum of human pathogens. A clear distinction must be made between 'healing clays' and those we have identified as antibacterial clays. The highly adsorptive properties of many clays may contribute to healing a variety of ailments, although they are not antibacterial. The antibacterial process displayed by the three identified clays is unknown. Therefore, we have investigated the mineralogical and chemical compositions of the antibacterial clays for comparison with non-antibacterial clays in an attempt to elucidate differences that may lead to identification of the antibacterial mechanism(s).The two French green clays used to treat Buruli ulcer, while similar in mineralogy, crystal size, and major element chemistry, have opposite effects on the bacterial populations tested. One clay deposit promoted bacterial growth whereas another killed the bacteria. The reasons for the difference in antibacterial properties thus far show that the bactericidal mechanism is not physical (e.g., an attraction between clay and bacteria), but by a chemical transfer or reaction. The chemical variables are still under investigation.Cation exchange experiments showed that the antibacterial component of the clay can be removed, implicating exchangeable cations in the antibacterial process. Furthermore, aqueous leachates of the antibacterial clays effectively kill the bacteria. Progressively heating the clay leads first to dehydration (200 degrees C), then dehydroxylation (550 degrees C or more), and finally to destruction of the clay mineral structure by (~900 degrees C). By identifying the elements lost after each heating step, and testing the bactericidal effect of the heated product, we eliminated many toxins from consideration (e.g., microbes, organic compounds, volatile elements) and identified several redox-sensitive refractory metals that are common among antibacterial clays. We conclude that the pH and oxidation state buffered by the clay mineral surfaces is key to controlling the solution chemistry and redox related reactions occurring at the bacterial cell wall.
Figures

References
-
- Abrahams PW, Parsons JA. Geophagy in the tropics: a literature review. The Geographical Journal. 1996;162:63–72.
-
- Adamis Z, Timar M. Investigations of the effects of quartz, aluminum silicates and colliery dusts on peritoneal macrophages in vitro. In: Brown RC, Gormley IP, Chamberlain M, Davies R, editors. The in vitro effects of mineral dusts. London: Academic Press; 1980. pp. 13–18.
-
- Adams LK, Lyon DY, McIntosh A, Alvarez PJ. Comparative toxicity of nano-scale TiO2, SiO2 and ZnO water suspensions. Water Science and Technology. 2006;54:327–334. - PubMed
-
- Altaner SP, Ylagan RF. Comparison of structural models of mixed-layer illite-smectite and reaction mechanisms of smectite illitization. Clays and Clay Minerals. 1997;45:517–533.
-
- Amofah GK, Sagoe-Moses C, Adjei-Acquah C, Frimpong EH. Epidemiology of Buruli ulcer in Amansie West district, Ghana. Transactions of the Royal Society of Tropical Medicine and Hygiene. 1993;87:644–645. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources