

Outcomes following temporal bone resection
- PMID: 20641083
- PMCID: PMC3951338
- DOI: 10.1002/lary.20999
Outcomes following temporal bone resection
Abstract
Objectives/hypothesis: To evaluate survival outcomes in patients undergoing temporal bone resection.
Study design: Retrospective review.
Methods: From 2002 to 2009 a total of 65 patients underwent temporal bone resection for epithelial (n = 47) and salivary (n = 18) skull base malignancies. Tumor characteristics, defect reconstruction, and postoperative course were assessed. Outcomes measured included disease-free survival and cancer recurrence.
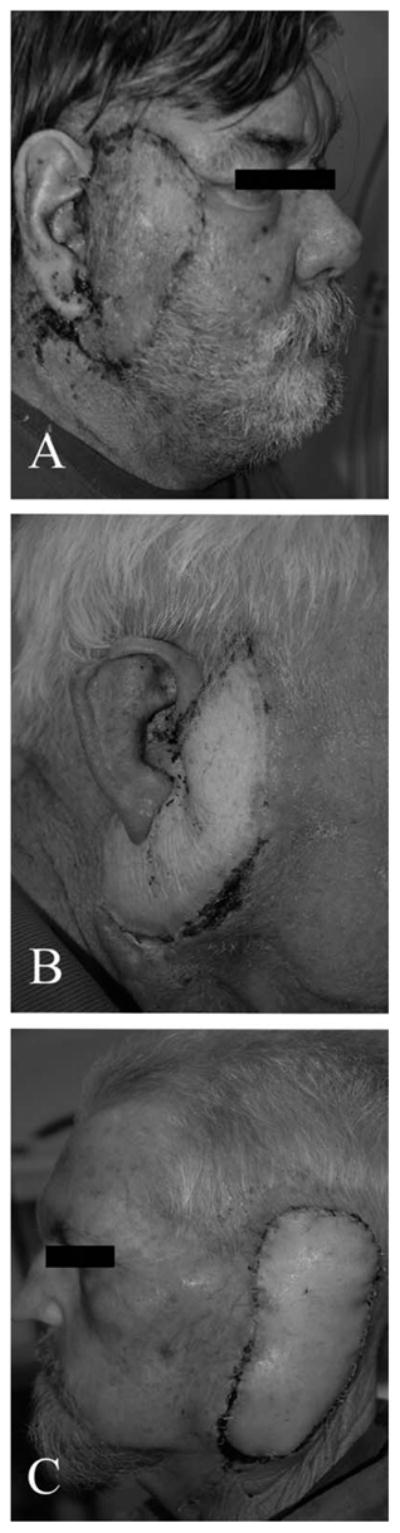
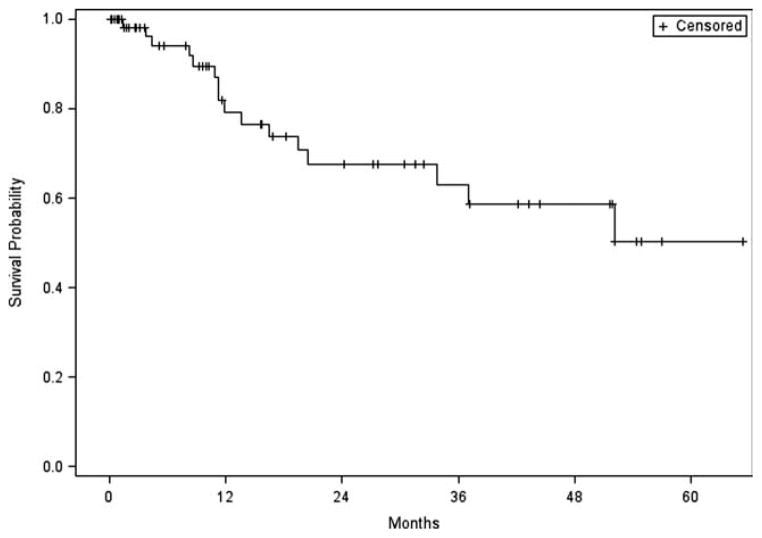
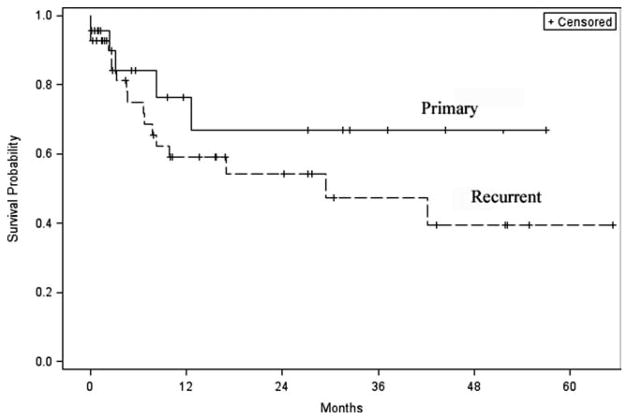
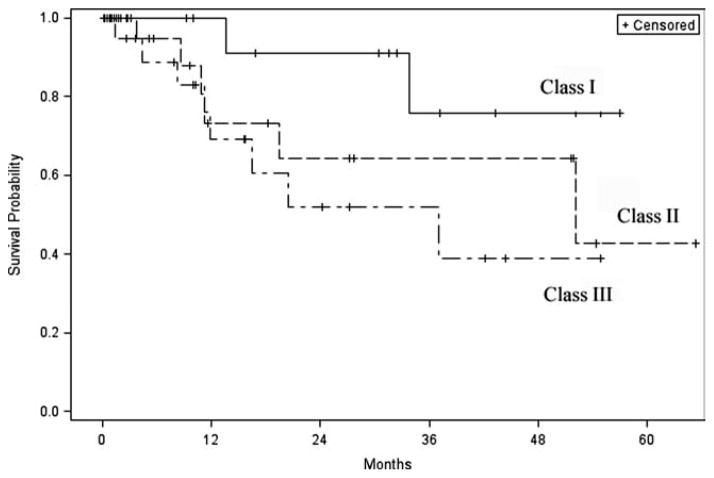
Results: The majority of patients presented with recurrent (65%), advanced stage (94%), cutaneous (72%), and squamous cell carcinoma (57%). Thirty-nine patients had perineural invasion (60%) and required facial nerve resection; 16 (25%) had intracranial extension. Local (n = 6), regional (n = 2), or free flap (n = 46) reconstruction was required in 80% of patients. Free flap donor sites included the anterolateral thigh (31%), radial forearm free flap (19%), rectus (35%), and latissimus (4%). The average hospital stay was 4.9 days (range, 1-28 days). The overall complication rate was 15% and included stroke (n = 4), cerebrospinal fluid leak (n = 2), hematoma formation (n = 1), infection (n = 1), flap loss (n = 1), and postoperative myocardial infarction (n = 1). A total of 22 patients (34%) developed cancer recurrence during the follow-up period (median, 10 months), 17 (77%) of whom presented with recurrent disease at the time of temporal bone resection. Two-year disease-free survival was 68%, and 5-year disease-free survival was 50%.
Conclusions: Aggressive surgical resection and reconstruction is recommended for primary and recurrent skull base malignancies with acceptable morbidity and improved disease-free survival.
Conflict of interest statement
The authors have no other funding, financial relationships, or conflicts of interest to disclose.
Figures
References
-
- Ward GE, Loch WE, Lawrence W., Jr Radical operation for carcinoma of the external auditory canal and middle ear. Am J Surg. 1951;82:169–178. - PubMed
-
- Parsons H, Lewis JS. Subtotal resection of the temporal bone for cancer of the ear. Cancer. 1954;7:995–1001. - PubMed
-
- Lewis JS. Temporal bone resection. Review of 100 cases. Arch Otolaryngol. 1975;101:23–25. - PubMed
-
- Goodwin WJ, Jesse RH. Malignant neoplasms of the external auditory canal and temporal bone. Arch Otolaryngol. 1980;106:675–679. - PubMed
-
- McGrew BM, Jackson CG, Redtfeldt RA. Lateral skull base malignancies. Neurosurg Focus. 2002;12:e8. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
