

Short- and medium-term outcomes after transcatheter pulmonary valve placement in the expanded multicenter US melody valve trial
- PMID: 20644013
- PMCID: PMC4240270
- DOI: 10.1161/CIRCULATIONAHA.109.921692
Short- and medium-term outcomes after transcatheter pulmonary valve placement in the expanded multicenter US melody valve trial
Abstract
Background: Transcatheter pulmonary valve placement is an emerging therapy for pulmonary regurgitation and right ventricular outflow tract obstruction in selected patients. The Melody valve was recently approved in the United States for placement in dysfunctional right ventricular outflow tract conduits.
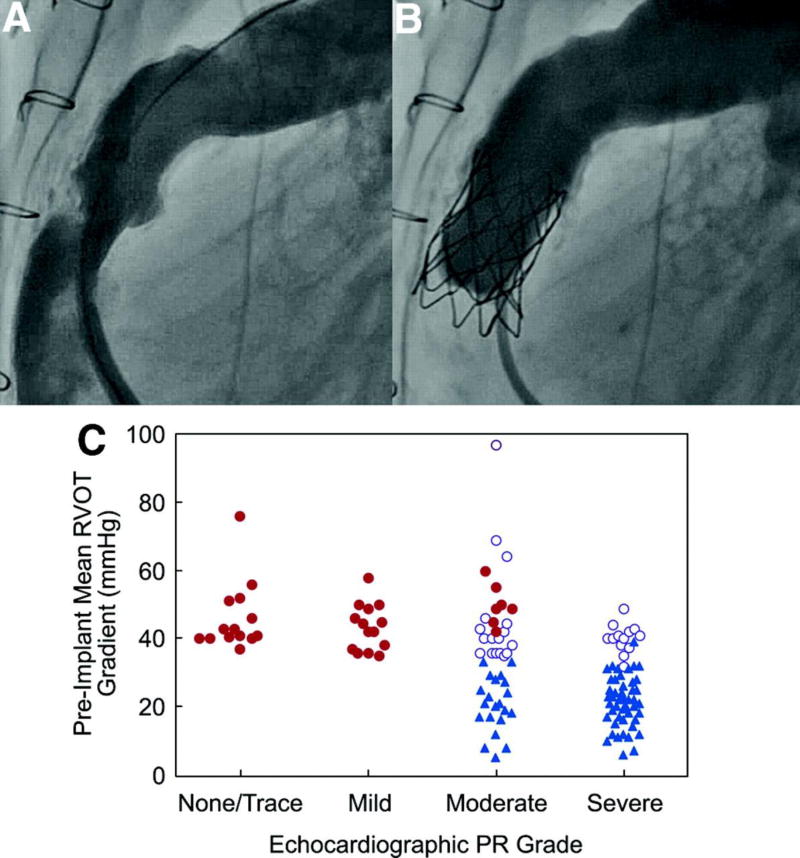
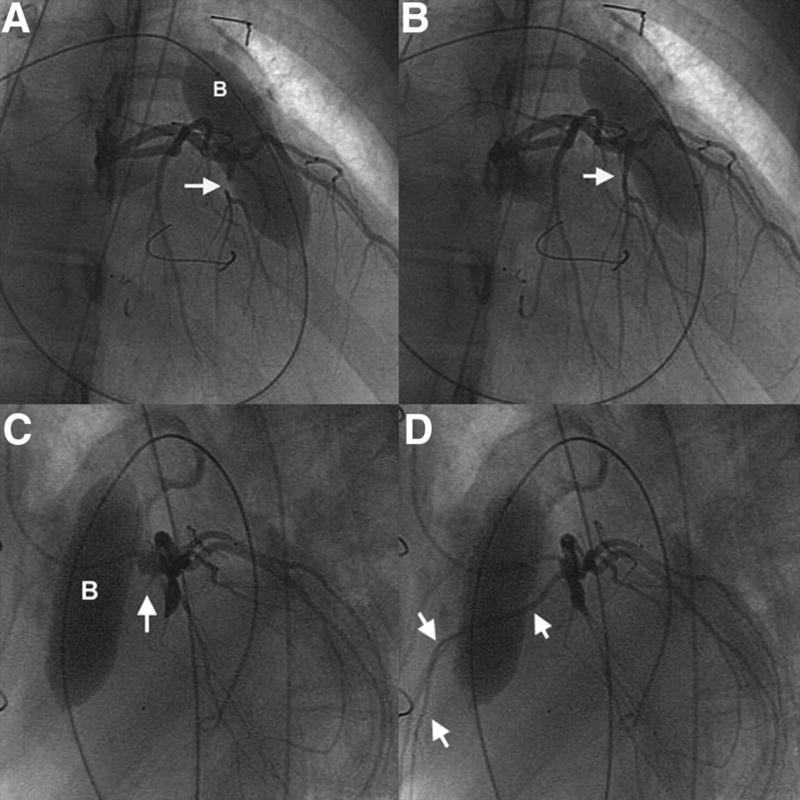
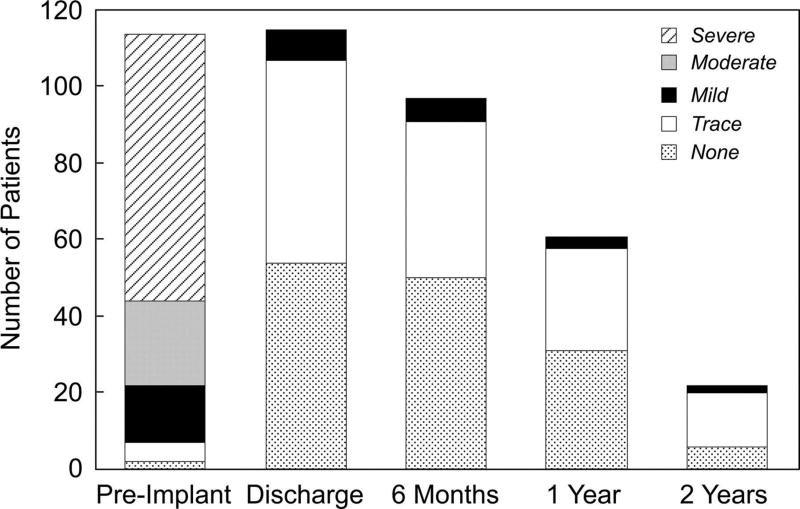
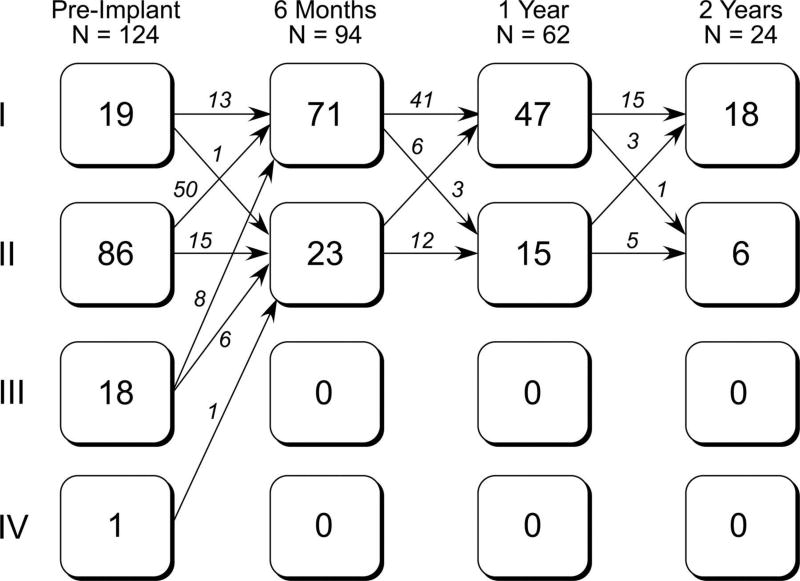
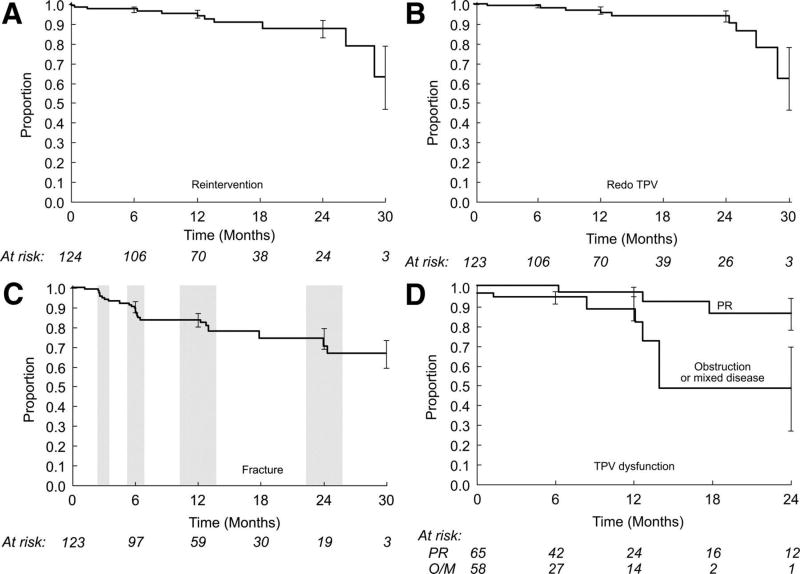
Methods and results: From January 2007 to August 2009, 136 patients (median age, 19 years) underwent catheterization for intended Melody valve implantation at 5 centers. Implantation was attempted in 124 patients; in the other 12, transcatheter pulmonary valve placement was not attempted because of the risk of coronary artery compression (n=6) or other clinical or protocol contraindications. There was 1 death from intracranial hemorrhage after coronary artery dissection, and 1 valve was explanted after conduit rupture. The median peak right ventricular outflow tract gradient was 37 mm Hg before implantation and 12 mm Hg immediately after implantation. Before implantation, pulmonary regurgitation was moderate or severe in 92 patients (81% with data); no patient had more than mild pulmonary regurgitation early after implantation or during follow-up (>or=1 year in 65 patients). Freedom from diagnosis of stent fracture was 77.8+/-4.3% at 14 months. Freedom from Melody valve dysfunction or reintervention was 93.5+/-2.4% at 1 year. A higher right ventricular outflow tract gradient at discharge (P=0.003) and younger age (P=0.01) were associated with shorter freedom from dysfunction.
Conclusions: In this updated report from the multicenter US Melody valve trial, we demonstrated an ongoing high rate of procedural success and encouraging short-term valve function. All reinterventions in this series were for right ventricular outflow tract obstruction, highlighting the importance of patient selection, adequate relief of obstruction, and measures to prevent and manage stent fracture. Clinical Trial Registration- URL: http://www.clinicaltrials.gov. Unique identifier: NCT00740870.
Figures
References
-
- Bonhoeffer P, Boudjemline Y, Saliba Z, Merckx J, Aggoun Y, Bonnet D, Acar P, Le Bidois J, Sidi D, Kachaner J. Percutaneous replacement of pulmonary valve in a right-ventricle to pulmonary-artery prosthetic conduit with valve dysfunction. Lancet. 2000;356:1403–1405. - PubMed
-
- Shimazaki Y, Blackstone EH, Kirklin JW. The natural history of isolated congenital pulmonary valve incompetence: surgical implications. Thorac Cardiovasc Surg. 1984;32:257–259. - PubMed
-
- Eyskens B, Reybrouck T, Bogaert J, Dymarkowsky S, Daenen W, Dumoulin M, Gewillig M. Homograft insertion for pulmonary regurgitation after repair of tetralogy of Fallot improves cardiorespiratory exercise performance. Am J Cardiol. 2000;85:221–225. - PubMed
-
- Gatzoulis MA, Balaji S, Webber SA, Siu SC, Hokanson JS, Poile C, Rosenthal M, Nakazawa M, Moller JH, Gillette PC, Webb GD, Redington AN. Risk factors for arrhythmia and sudden cardiac death late after repair of tetralogy of Fallot: a multicentre study. Lancet. 2000;356:975–981. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
