

Absence of biallelic TCRgamma deletion predicts early treatment failure in pediatric T-cell acute lymphoblastic leukemia
- PMID: 20644084
- PMCID: PMC2940399
- DOI: 10.1200/JCO.2010.28.3390
Absence of biallelic TCRgamma deletion predicts early treatment failure in pediatric T-cell acute lymphoblastic leukemia
Abstract
Purpose: To identify children with T-cell acute lymphoblastic leukemia (T-ALL) at high risk of induction chemotherapy failure by using DNA copy number analysis of leukemic cells collected at diagnosis.
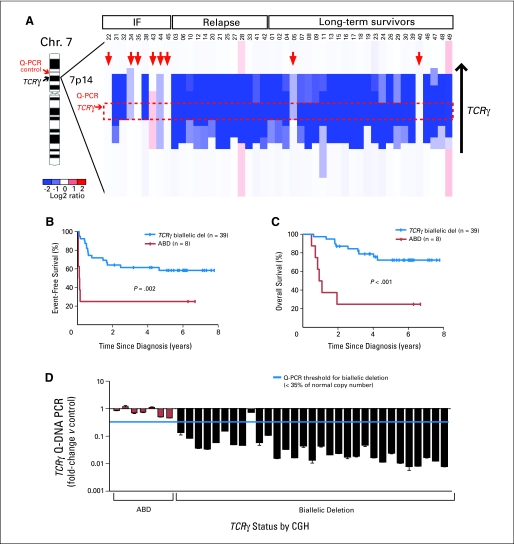
Patients and methods: Array comparative genomic hybridization (CGH) was performed on genomic DNA extracted from diagnostic lymphoblasts from 47 children with T-ALL treated on Children's Oncology Group Study P9404 or Dana-Farber Cancer Institute Protocol 00-01. These samples represented nine patients who did not achieve an initial complete remission, 13 who relapsed, and 25 who became long-term, event-free survivors. The findings were confirmed in an independent cohort of patients by quantitative DNA polymerase chain reaction (DNA-PCR), an assay that is well suited for clinical application.
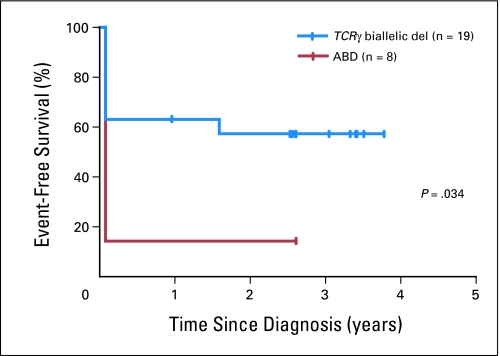
Results: Analysis of the CGH findings in patients in whom induction chemotherapy failed compared with those in whom induction chemotherapy was successful identified the absence of biallelic TCRgamma locus deletion (ABD), a characteristic of early thymocyte precursors before V(D)J recombination, as the most robust predictor of induction failure (P < .001). This feature was also associated with markedly inferior event-free (P = .002) and overall survival (P < .001) rates: 25% versus 58% and 25% versus 72%, respectively. Using a rapid and inexpensive quantitative DNA-PCR assay, we validated ABD as a predictor of a poor response to induction chemotherapy in an independent series of patients.
Conclusion: Lymphoblasts from children with T-ALL should be evaluated at diagnosis for deletion within the TCRgamma locus. Patients lacking biallelic deletion, which confers a high probability of induction failure with contemporary therapy, should be assigned to alternative therapy in the context of a prospective clinical trial.
Conflict of interest statement
Authors' disclosures of potential conflicts of interest and author contributions are found at the end of this article.
Figures
References
-
- Annino L, Vegna ML, Camera A, et al. Treatment of adult acute lymphoblastic leukemia (ALL): Long-term follow-up of the GIMEMA ALL 0288 randomized study. Blood. 2002;99:863–871. - PubMed
-
- Goldberg JM, Silverman LB, Levy DE, et al. Childhood T-cell acute lymphoblastic leukemia: The Dana-Farber Cancer Institute acute lymphoblastic leukemia consortium experience. J Clin Oncol. 2003;21:3616–3622. - PubMed
-
- Einsiedel HG, von Stackelberg A, Hartmann R, et al. Long-term outcome in children with relapsed ALL by risk-stratified salvage therapy: Results of trial acute lymphoblastic leukemia-relapse study of the Berlin-Frankfurt-Münster Group 87. J Clin Oncol. 2005;23:7942–7950. - PubMed
Publication types
MeSH terms
Grants and funding
- 1K08CA133103/CA/NCI NIH HHS/United States
- CA98543/CA/NCI NIH HHS/United States
- NCI 5P01CA68484/CA/NCI NIH HHS/United States
- R01 CA129382/CA/NCI NIH HHS/United States
- CA114766/CA/NCI NIH HHS/United States
- K08 CA133103/CA/NCI NIH HHS/United States
- L40 CA124083/CA/NCI NIH HHS/United States
- R01CA120196/CA/NCI NIH HHS/United States
- R01 CA120196/CA/NCI NIH HHS/United States
- CA98413/CA/NCI NIH HHS/United States
- P01 CA068484/CA/NCI NIH HHS/United States
- U10 CA098413/CA/NCI NIH HHS/United States
- U24 CA114766/CA/NCI NIH HHS/United States
- R01CA129382/CA/NCI NIH HHS/United States
- U10 CA098543/CA/NCI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
