

The empirical basis for determinations of medical futility
- PMID: 20645019
- PMCID: PMC2955478
- DOI: 10.1007/s11606-010-1445-3
The empirical basis for determinations of medical futility
Abstract
Background: Decisions to limit treatment in critically ill patients often rely on publications that make claims of futility based on outcome data. Our objective was to systematically review the criteria for futility and the strength of empirical evidence across clinical studies that purport to support or refute claims of futility.
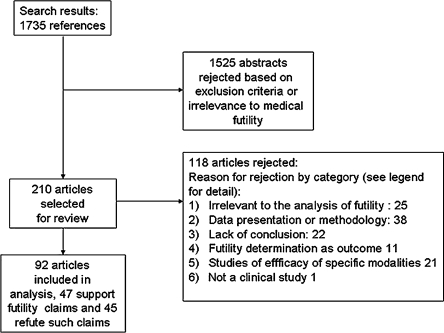
Methods: The MEDLINE database was searched for relevant articles published between 1980 and 2008. Selected studies reported original outcome data in critically ill or cardiac arrest patients and claimed that these data can support or refute decisions to limit treatment in comparable patients. Two authors independently abstracted data on patient characteristics, intervention, outcomes, cost, and design.
Results: Forty seven studies supporting a claim of futility and 45 refuting it were reviewed. Median point estimate for adverse outcome in studies supporting claims of futility was 100% (range 75% to 100%); median lower 95% confidence limit was 91% (range 48% to 99%). Explicit thresholds for futility were missing in 88% of articles. The original criteria for quantitative futility were fulfilled by only 28% of data, and almost exclusively in studies of cardiopulmonary resuscitation (CPR) for cardiac arrest. Substantial statistical overlap was observed between data brought in support of futility claims and data brought to refute them.
Conclusions: Most studies that purport to guide determinations of futility are based on insufficient data to provide statistical confidence for clinical decision-making. They usually lack explicit a priori thresholds for determination of futility. Many studies draw disparate conclusions based on statistically similar data. In most circumstances these problems preclude confident determinations of futility.
Figures

References
-
- Hakim RB, Teno JM, Harrell FE, Jr, et al. Factors associated with do-not-resuscitate orders: patients' preferences, prognoses, and physicians' judgments. SUPPORT Investigators. Study to Understand Prognoses and Preferences for Outcomes and Risks of Treatment. Ann Intern Med. 1996;125(4):284–93. - PubMed
-
- A controlled trial to improve care for seriously ill hospitalized patients. The study to understand prognoses and preferences for outcomes and risks of treatments (SUPPORT). The SUPPORT Principal Investigators. JAMA. 1995; 274(20):1591-8. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
