

A multicenter randomized clinical trial investigating the cost-effectiveness of treatment strategies with or without antibiotics for uncomplicated acute diverticulitis (DIABOLO trial)
- PMID: 20646266
- PMCID: PMC2919453
- DOI: 10.1186/1471-2482-10-23
A multicenter randomized clinical trial investigating the cost-effectiveness of treatment strategies with or without antibiotics for uncomplicated acute diverticulitis (DIABOLO trial)
Abstract
Background: Conservative treatment of uncomplicated or mild diverticulitis usually includes antibiotic therapy. It is, however, uncertain whether patients with acute diverticulitis indeed benefit from antibiotics. In most guidelines issued by professional organizations antibiotics are considered mandatory in the treatment of mild diverticulitis. This advice lacks evidence and is merely based on experts' opinion. Adverse effects of the use of antibiotics are well known, including allergic reactions, development of bacterial resistance to antibiotics and other side-effects.
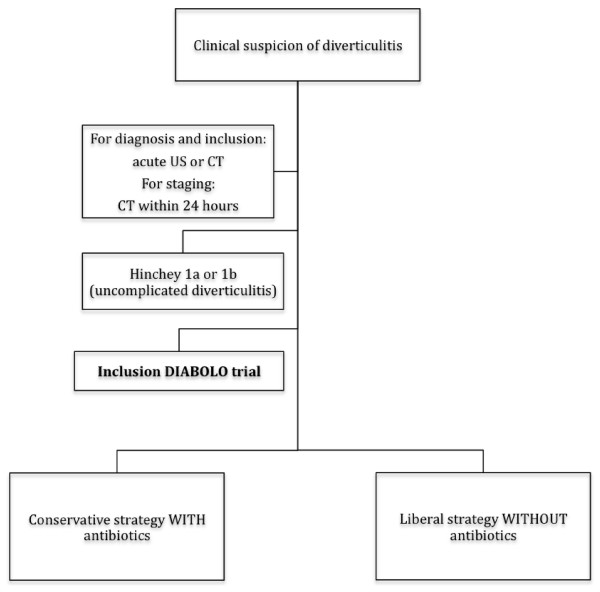
Methods: A randomized multicenter pragmatic clinical trial comparing two treatment strategies for uncomplicated acute diverticulitis. I) A conservative strategy with antibiotics: hospital admission, supportive measures and at least 48 hours of intravenous antibiotics which subsequently are switched to oral, if tolerated (for a total duration of antibiotic treatment of 10 days). II) A liberal strategy without antibiotics: admission only if needed on clinical grounds, supportive measures only. Patients are eligible for inclusion if they have a diagnosis of acute uncomplicated diverticulitis as demonstrated by radiological imaging. Only patients with stages 1a and 1b according to Hinchey's classification or "mild" diverticulitis according to the Ambrosetti criteria are included. The primary endpoint is time-to-full recovery within a 6-month follow-up period. Full recovery is defined as being discharged from the hospital, with a return to pre-illness activities, and VAS score below 4 without the use of daily pain medication. Secondary endpoints are proportion of patients who develop complicated diverticulitis requiring surgery or non-surgical intervention, morbidity, costs, health-related quality of life, readmission rate and acute diverticulitis recurrence rate. In a non-inferiority design 264 patients are needed in each study arm to detect a difference in time-to-full recovery of 5 days or more with a power of 85% and a confidence level of 95%. With an estimated one percent of patients lost to follow up, a total of 533 patients will be included.
Conclusion: A clinically relevant difference of more than 5 days in time-to-full recovery between the two treatment strategies is not expected. The liberal strategy without antibiotics and without the strict requirement for hospital admission is anticipated to be more a more cost-effective approach.
Trial registration number: NCT01111253.
References
-
- Mendeloff AI. Thoughts on epidemiology of diverticular disease. Clin Gastroenterel. 1986;15:855–77. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
