

Case Reports
doi: 10.1186/1749-8090-5-55.
Inflammatory myofibroblastic tumor of the lung--a case report
Affiliations
- PMID: 20646317
- PMCID: PMC2915987
- DOI: 10.1186/1749-8090-5-55
Item in Clipboard
Case Reports
Inflammatory myofibroblastic tumor of the lung--a case report
J Cardiothorac Surg.
.
Abstract
A 45-year-old man presented with a six-month history of progressive dyspnea with productive cough and wheezing. The patient was a heavy smoker and had a history of tongue cancer, hypertension, and asthma. Chest X-ray and computed tomography showed a mass lesion in the left hilar region and total collapse of the upper left lobe of the lung. Bronchoscopy revealed a whitish solid tumor obstructing the left upper lobe bronchus. Positron emission tomography showed increased tracer uptake in the lesion. A thoracoscopic lobectomy of the left upper lobe of the lung was performed. The final pathologic diagnosis was inflammatory myofibroblastic tumor.
Figures
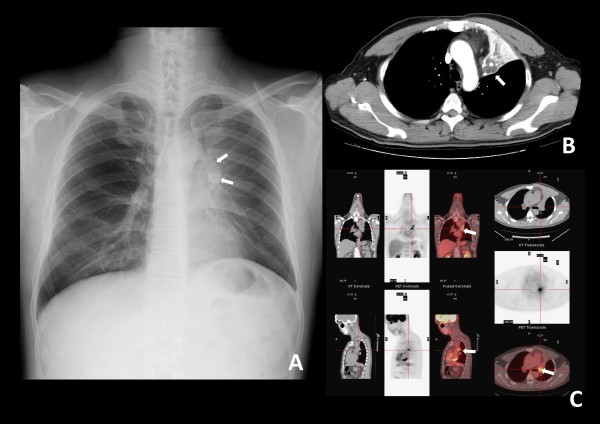
(A) Chest plain film. A protruding mass shadow is seen in the left hilar region. The shadow of the left bronchus stops at the mass. Costodiaphragmatic angles are clear. There is increased density over the left lung field with elevation of the left side of the diaphragm. These findings are indicative of a hilar mass obstructing the bronchus with collapse of the left upper lobe of lung. (B) Contrast computed tomography (CT) image, distal part of the tumor. The distal bronchus is dilated and filled with secretions. The margin between the lung parenchyma and tumor is indistinct. (C) Positron emission tomography (PET) and CT, proximal part of the tumor. An endobronchial tumor with high tracer uptake and clear margins is visible.
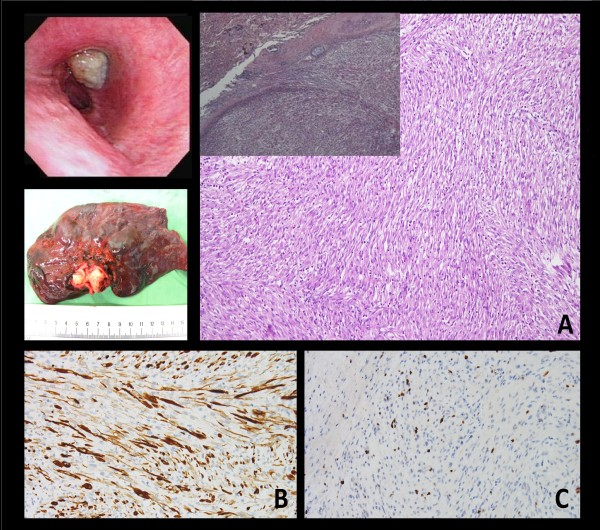
Bronchoscopic exam shows a whitish tumor obstructing the left upper bronchus. Gross. The tumor impacted the whole bronchus with clear margins. Microscopically, the biopsy specimen is composed of spindle cells with fibroblastic and myofibroblastic differentiation arrayed in fascicles. (A) The tumor is mostly limited within the bronchi. In a few foci, pushing of tumor margin to the lung parenchyma is noted (×20; ×100). Immunohistochemical study demonstrated (B) vimentin (+) (×200), and (C) cytokeratin (focal +), (×200).
Similar articles
-
A case of pulmonary inflammatory myofibroblastic tumor treated with bronchoscopic therapy plus lobectomy.J Cardiothorac Surg. 2021 May 26;16(1):144. doi: 10.1186/s13019-021-01528-5. J Cardiothorac Surg. 2021. PMID: 34039398 Free PMC article.
-
Pulmonary inflammatory myofibroblastic tumor: a case report.Asian Cardiovasc Thorac Ann. 2018 May;26(4):317-319. doi: 10.1177/0218492318770845. Epub 2018 Apr 12. Asian Cardiovasc Thorac Ann. 2018. PMID: 29649880
-
Successful sleeve lobectomy of pediatric inflammatory myofibroblastic tumor.Pediatr Int. 2016 Oct;58(10):1087-1089. doi: 10.1111/ped.13079. Pediatr Int. 2016. PMID: 27804248
-
Inflammatory pseudotumor suspected of lung cancer treated by thoracoscopic resection.Ann Thorac Cardiovasc Surg. 2011;17(1):48-52. doi: 10.5761/atcs.cr.09.01488. Ann Thorac Cardiovasc Surg. 2011. PMID: 21587129 Review.
-
[A resected case of pulmonary plasma cell granuloma infiltrating the pericardium].Nihon Kyobu Geka Gakkai Zasshi. 1994 Sep;42(9):1399-403. Nihon Kyobu Geka Gakkai Zasshi. 1994. PMID: 7989806 Review. Japanese.
Cited by
-
Inflammatory myofibroblastic tumour of the bladder: Case report and review of the literature.Can Urol Assoc J. 2013 Mar-Apr;7(3-4):E237-40. doi: 10.5489/cuaj.544. Can Urol Assoc J. 2013. PMID: 23671533 Free PMC article.
-
Inflammatory Myofibroblastic Tumor of the Lung: An Incidental Finding of a Pediatric Case.Ann Thorac Surg Short Rep. 2024 Mar 7;2(3):477-480. doi: 10.1016/j.atssr.2024.02.006. eCollection 2024 Sep. Ann Thorac Surg Short Rep. 2024. PMID: 39790401 Free PMC article.
-
Inflammatory Endobronchial Myofibroblastic Tumor: A Case Report.Taehan Yongsang Uihakhoe Chi. 2020 Jan;81(1):219-224. doi: 10.3348/jksr.2020.81.1.219. Epub 2020 Jan 31. Taehan Yongsang Uihakhoe Chi. 2020. PMID: 36238110 Free PMC article.
-
Imaging observations of pulmonary inflammatory myofibroblastic tumors in patients over 40 years old.Oncol Lett. 2015 Apr;9(4):1877-1884. doi: 10.3892/ol.2015.2923. Epub 2015 Feb 2. Oncol Lett. 2015. PMID: 25789060 Free PMC article.
-
A rare tumor of the lung: inflammatory myofibroblastic tumor.Diagn Pathol. 2012 Jul 17;7:83. doi: 10.1186/1746-1596-7-83. Diagn Pathol. 2012. PMID: 22805416 Free PMC article.
References
-
- Pettinato G, Manivel JC, Derosa N, Dehner LP. Inflammatory Myofibroblastic Tumor (Plasma-Cell Granuloma) - Clinicopathological Study Of 20 Cases With Immunohistochemical And Ultrastructural Observations. American Journal of Clinical Pathology. 1990;94:538–546. - PubMed
-
- Rasalkar DD, Chu WCW, To KF, Cheng FWT, Li CK. Radiological Appearance of Inflammatory Myofibroblastic Tumour. Pediatric Blood & Cancer. 2010;54:1029–1031. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
