

Candidate dosimetric predictors of long-term swallowing dysfunction after oropharyngeal intensity-modulated radiotherapy
- PMID: 20646872
- PMCID: PMC4034521
- DOI: 10.1016/j.ijrobp.2009.10.002
Candidate dosimetric predictors of long-term swallowing dysfunction after oropharyngeal intensity-modulated radiotherapy
Abstract
Purpose: To investigate long-term swallowing function in oropharyngeal cancer patients treated with intensity-modulated radiotherapy (IMRT), and to identify novel dose-limiting criteria predictive for dysphagia.
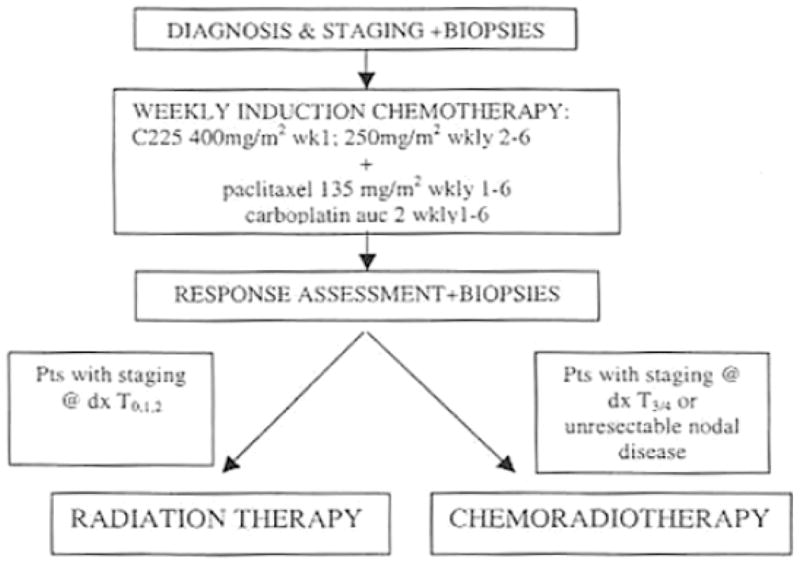
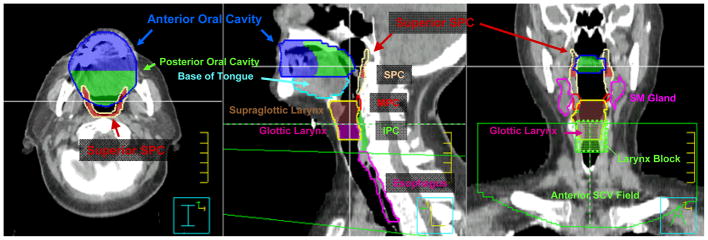
Methods and materials: Thirty-one patients with Stage IV oropharyngeal squamous carcinoma enrolled on a Phase II trial were prospectively evaluated by modified barium swallow studies at baseline, and 6, 12, and 24 months post-IMRT treatment. Candidate dysphagia-associated organs at risk were retrospectively contoured into original treatment plans. Twenty-one (68%) cases were base of tongue and 10 (32%) were tonsil. Stage distribution was T1 (12 patients), T2 (10), T3 (4), T4 (2), and TX (3), and N2 (24), N3 (5), and NX (2). Median age was 52.8 years (range, 42-78 years). Thirteen patients (42%) received concurrent chemotherapy during IMRT. Thirteen (42%) were former smokers. Mean dose to glottic larynx for the cohort was limited to 18 Gy (range, 6-39 Gy) by matching IMRT to conventional low-neck fields.
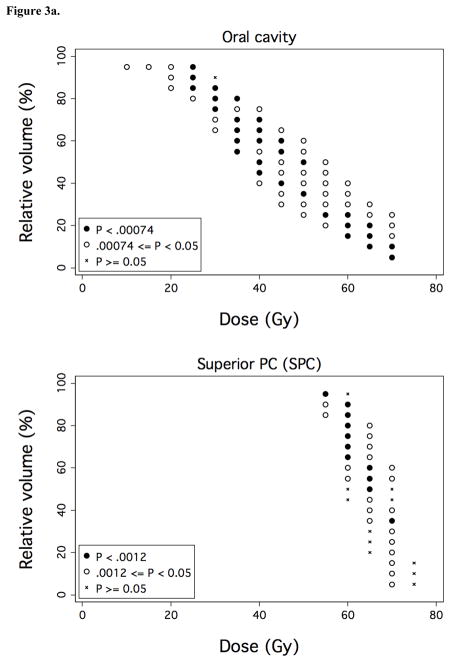
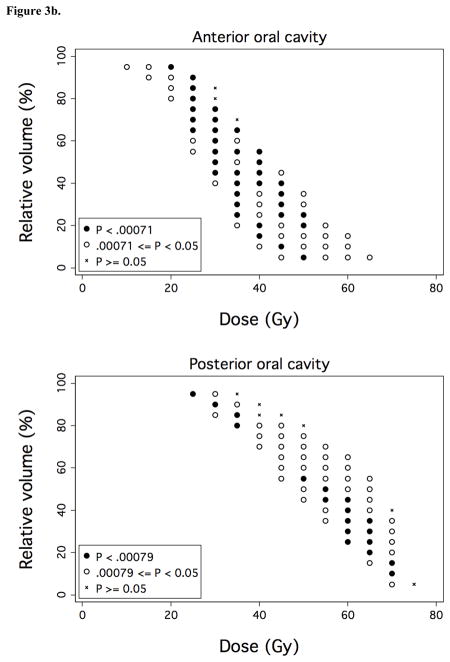
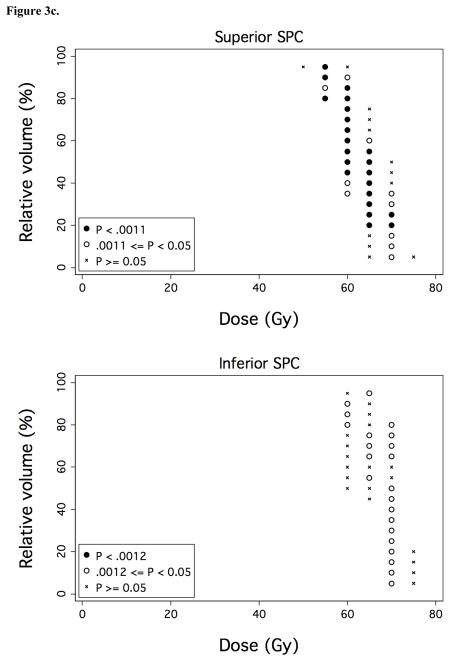
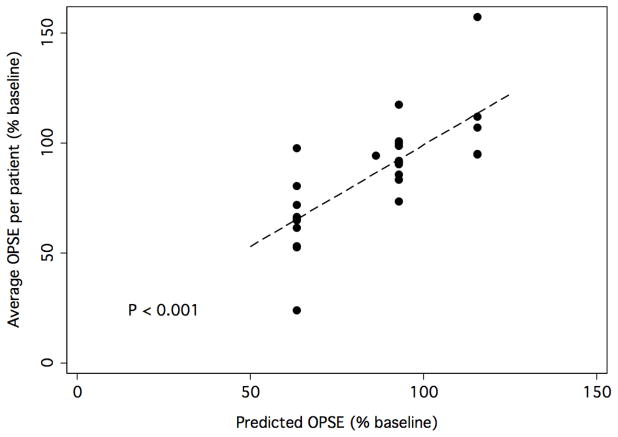
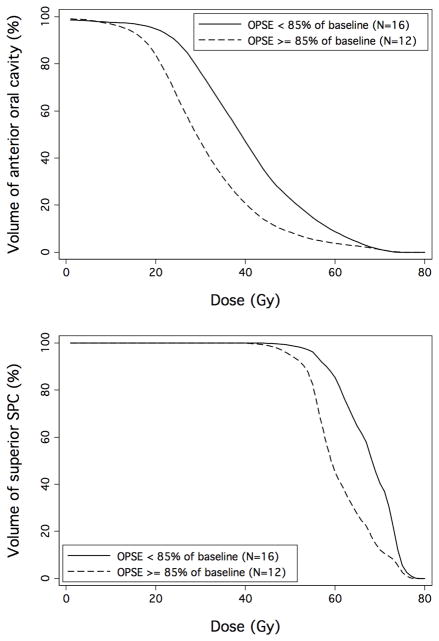
Results: Dose-volume constraints (V30 < 65% and V35 < 35% for anterior oral cavity and V55 < 80% and V65 < 30% for high superior pharyngeal constrictors) predictive for objective swallowing dysfunction were identified by univariate and multivariate analyses. Aspiration and feeding tube dependence were observed in only 1 patient at 24 months.
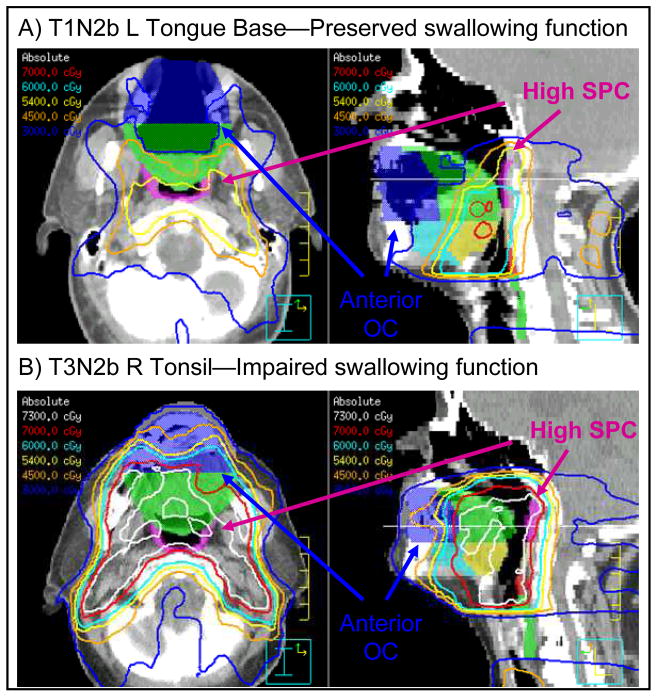
Conclusions: In the context of glottic laryngeal shielding, we describe candidate oral cavity and superior pharyngeal constrictor organs at risk and dose-volume constraints associated with preserved long-term swallowing function; these constraints are currently undergoing prospective validation. Strict protection of the glottic larynx via beam-split IMRT techniques promises to make chronic aspiration an uncommon outcome.
Copyright © 2010 Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures
References
-
- Eisbruch A, Lyden T, Bradford CR, et al. Objective assessment of swallowing dysfunction and aspiration after radiation concurrent with chemotherapy for head-and-neck cancer. Int J Radiat Oncol Biol Phys. 2002;53:23–28. - PubMed
-
- Rademaker AW, Vonesh EF, Logemann JA, et al. Eating ability in head and neck cancer patients after treatment with chemoradiation: a 12-month follow-up study accounting for dropout. Head Neck. 2003;25:1034–1041. - PubMed
-
- Mittal BB, Pauloski BR, Haraf DJ, et al. Swallowing dysfunction--preventative and rehabilitation strategies in patients with head-and-neck cancers treated with surgery, radiotherapy, and chemotherapy: a critical review. Int J Radiat Oncol Biol Phys. 2003;57:1219–1230. - PubMed
-
- Chao KS, Wippold FJ, Ozyigit G, et al. Determination and delineation of nodal target volumes for head-and-neck cancer based on patterns of failure in patients receiving definitive and postoperative IMRT. Int J Radiat Oncol Biol Phys. 2002;53:1174–1184. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
