

Potential biomarkers for hypoxic-ischemic encephalopathy
- PMID: 20646975
- PMCID: PMC2930085
- DOI: 10.1016/j.siny.2010.05.007
Potential biomarkers for hypoxic-ischemic encephalopathy
Abstract
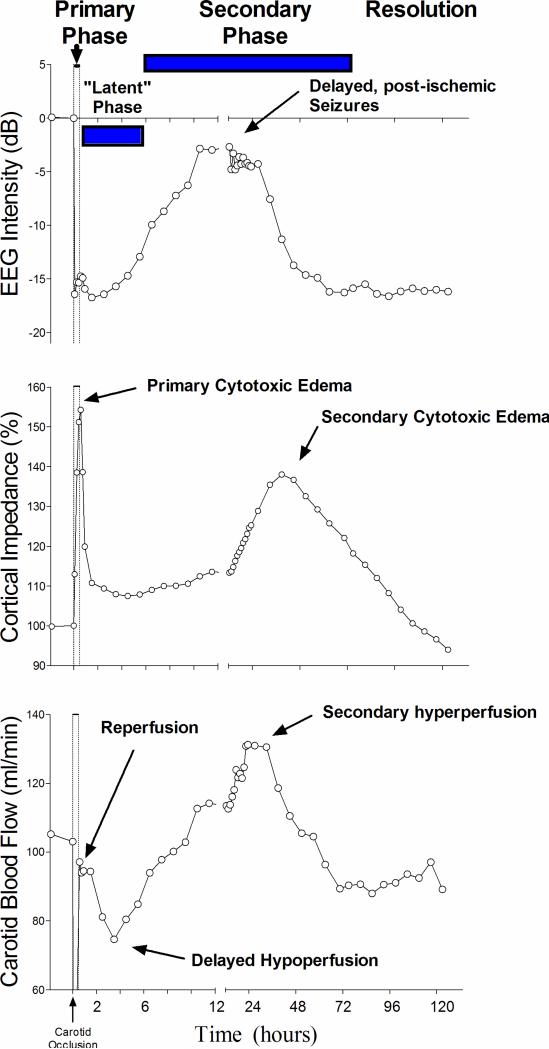
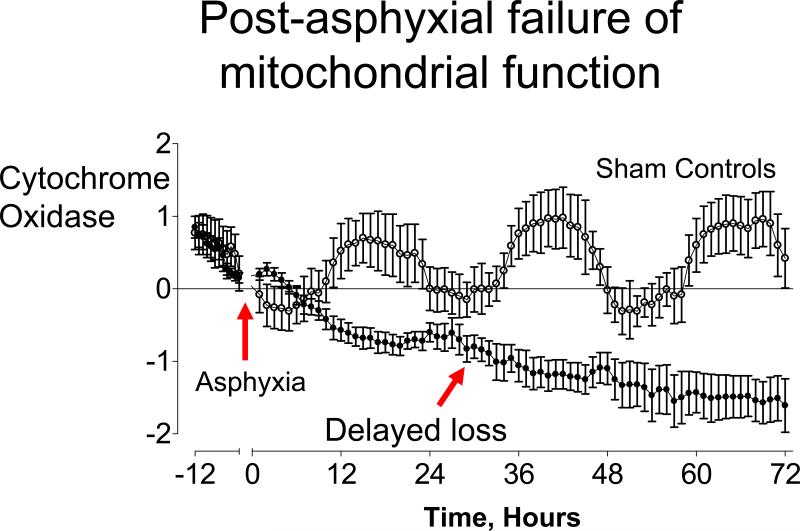
Cerebral hypothermia reduces brain injury and improves behavioral recovery after hypoxia-ischemia (HI) at birth. However, using current enrolment criteria many infants are not helped, and conversely, a significant proportion of control infants survive without disability. In order to further improve treatment we need better biomarkers of injury. A 'true' biomarker for the phase of evolving, 'treatable' injury would allow us to identify not only whether infants are at risk of damage, but also whether they are still able to benefit from intervention. Even a less specific measure that allowed either more precise early identification of infants at risk of adverse neurodevelopmental outcome would reduce the variance of outcome of trials, improving trial power while reducing the number of infants unnecessarily treated. Finally, valid short-term surrogates for long term outcome after treatment would allow more rapid completion of preliminary evaluation and thus allow new strategies to be tested more rapidly. Experimental studies have demonstrated that there is a relatively limited 'window of opportunity' for effective treatment (up to about 6-8h after HI, the 'latent phase'), before secondary cell death begins. We critically evaluate the utility of proposed biochemical, electronic monitoring, and imaging biomarkers against this framework. This review highlights the two central limitations of most presently available biomarkers: that they are most precise for infants with severe injury who are already easily identified, and that their correlation is strongest at times well after the latent phase, when injury is no longer 'treatable'. This is an important area for further research.
Copyright © 2010 Elsevier Ltd. All rights reserved.
Figures

References
-
- Bennet L, Dean JM, Gunn AJ. The pathogenesis of preterm brain injury. In: Stevenson DK, Benitz WE, Sunshine P, Druzin ML, editors. Fetal and neonatal brain injury: mechanisms, management, and the risks of practice. 4th edition Cambridge University Press; Cambridge: 2009. pp. 48–57.
-
- Gunn AJ, Bennet L. Timing of injury in the fetus and neonate. Curr Opin Obstet Gynecol. 2008;20:175–81. - PubMed
-
- Shankaran S, Laptook AR, Ehrenkranz RA, et al. Whole-body hypothermia for neonates with hypoxic–ischemic encephalopathy. N Engl J Med. 2005;353:1574–84. - PubMed
-
- Eicher DJ, Wagner CL, Katikaneni LP, et al. Moderate hypothermia in neonatal encephalopathy: efficacy outcomes. Pediatr Neurol. 2005;32:11–17. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
