

Early versus standard antiretroviral therapy for HIV-infected adults in Haiti
- PMID: 20647201
- PMCID: PMC3676927
- DOI: 10.1056/NEJMoa0910370
Early versus standard antiretroviral therapy for HIV-infected adults in Haiti
Abstract
Background: For adults with human immunodeficiency virus (HIV) infection who have CD4+ T-cell counts that are greater than 200 and less than 350 per cubic millimeter and who live in areas with limited resources, the optimal time to initiate antiretroviral therapy remains uncertain.
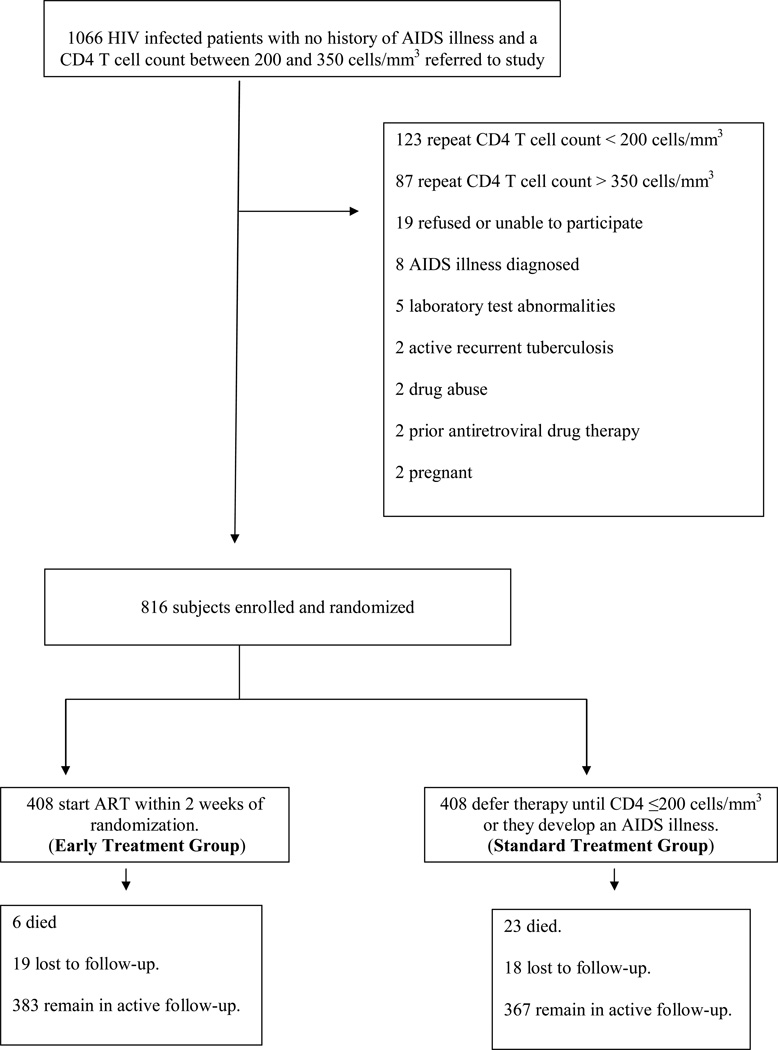
Methods: We conducted a randomized, open-label trial of early initiation of antiretroviral therapy, as compared with the standard timing for initiation of therapy, among HIV-infected adults in Haiti who had a confirmed CD4+ T-cell count that was greater than 200 and less than 350 per cubic millimeter at baseline and no history of an acquired immunodeficiency syndrome (AIDS) illness. The primary study end point was survival. The early-treatment group began taking zidovudine, lamivudine, and efavirenz therapy within 2 weeks after enrollment. The standard-treatment group started the same regimen of antiretroviral therapy when their CD4+ T-cell count fell to 200 per cubic millimeter or less or when clinical AIDS developed. Participants in both groups underwent monthly follow-up assessments and received isoniazid and trimethoprim-sulfamethoxazole prophylaxis with nutritional support.
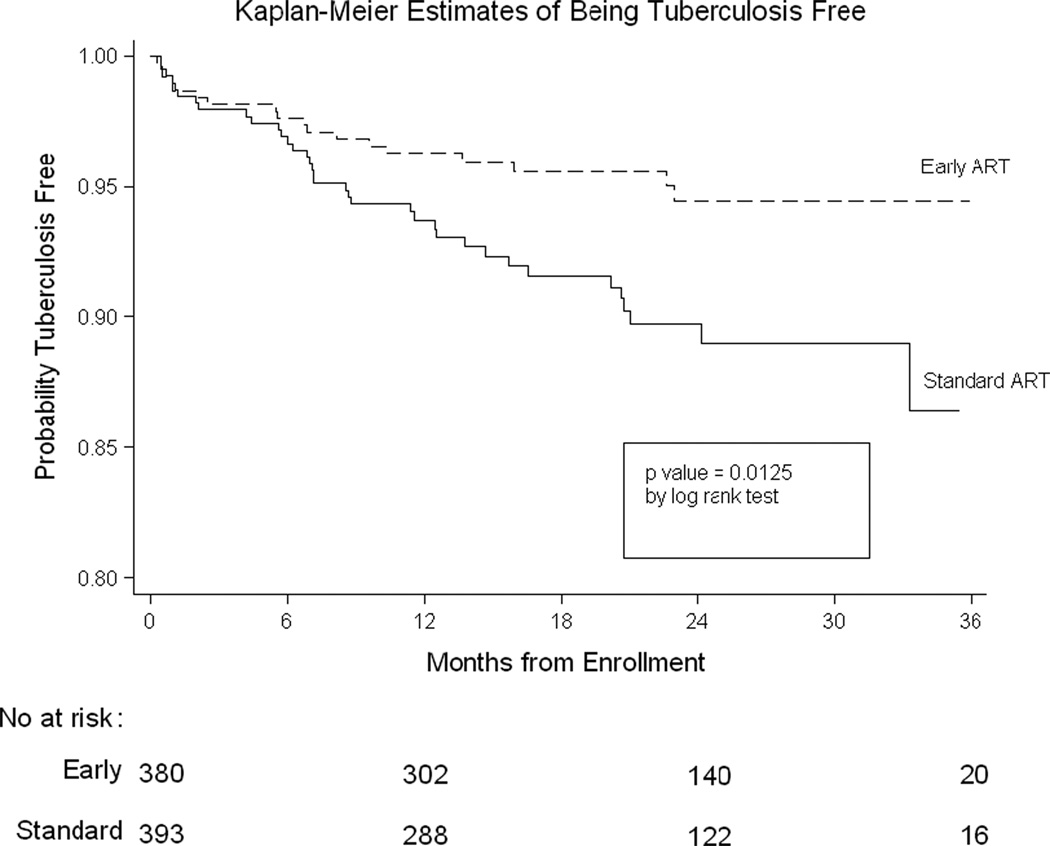
Results: Between 2005 and 2008, a total of 816 participants--408 per group--were enrolled and were followed for a median of 21 months. The CD4+ T-cell count at enrollment was approximately 280 per cubic millimeter in both groups. There were 23 deaths in the standard-treatment group, as compared with 6 in the early-treatment group (hazard ratio with standard treatment, 4.0; 95% confidence interval [CI], 1.6 to 9.8; P=0.001). There were 36 incident cases of tuberculosis in the standard-treatment group, as compared with 18 in the early-treatment group (hazard ratio, 2.0; 95% CI, 1.2 to 3.6; P=0.01).
Conclusions: Early initiation of antiretroviral therapy decreased the rates of death and incident tuberculosis. Access to antiretroviral therapy should be expanded to include all HIV-infected adults who have CD4+ T-cell counts of less than 350 per cubic millimeter, including those who live in areas with limited resources. (ClinicalTrials.gov number, NCT00120510.)
2010 Massachusetts Medical Society
Figures


References
-
- World Health Organization. Scaling up Antiretroviral Therapy in resource-limited settings. Geneva: World Health Organization; 2004.
-
- World Health Organization. Antiretroviral Therapy for HIV Infection in Adults and Adolescents: Recommendations for a Public Health Approach, 2006 Revision. Geneva: World Health Organization; 2006. - PubMed
-
- Guidelines for the use of antiretroviral agents in HIV-1-infected adults and adolescents. Department of Health and Human Services; 2008. Nov 3, [Accessed June 1, 2009]. Panel on Antiretroviral Guidelines for Adults and Adolescents; pp. 1–139.pp. 20–26. Available at http://www.aidsinfo.nih.gov/ContentFiles/AdultandAdolescentGL.pdf.
-
- Hammer SM, Eron JJ, Jr, Reiss P, Schooley RT, Thompson MA, Walmsley S, Cahn P, Fischl MA, Gatell JM, Hirsch MS, Jacobsen DM, Montaner JS, Richman DD, Yeni PG, Volberding PA International AIDS Society-USA. Antiretroviral treatment of adult HIV infection: 2008 recommendations of the International AIDS Society–USA panel. JAMA. 2008;300:555–570. - PubMed
-
- European AIDS Clinical Society (EACS) [Accessed September 1, 2009];Guidelines for the Clinical Management and Treatment of HIV Infected Adults in Europe. Available at: http://www.europeanaidsclinicalsociety.org/guidelines.asp.
Publication types
MeSH terms
Substances
Associated data
Grants and funding
- AI51966/AI/NIAID NIH HHS/United States
- TW006896/TW/FIC NIH HHS/United States
- UM1 AI069421/AI/NIAID NIH HHS/United States
- U2R TW006901/TW/FIC NIH HHS/United States
- K24 AI051966/AI/NIAID NIH HHS/United States
- U2R TW006896/TW/FIC NIH HHS/United States
- U01 AI069421/AI/NIAID NIH HHS/United States
- TW006901/TW/FIC NIH HHS/United States
- AI69421/AI/NIAID NIH HHS/United States
- AI58257/AI/NIAID NIH HHS/United States
- U01 AI058257/AI/NIAID NIH HHS/United States
- D43 TW000018/TW/FIC NIH HHS/United States
- TW 00018/TW/FIC NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials