

Is there a causal relationship between the hypoxia-ischaemia associated with cardiorespiratory arrest and subdural haematomas? An observational study
- PMID: 20647510
- PMCID: PMC3473414
- DOI: 10.1259/bjr/36871113
Is there a causal relationship between the hypoxia-ischaemia associated with cardiorespiratory arrest and subdural haematomas? An observational study
Abstract
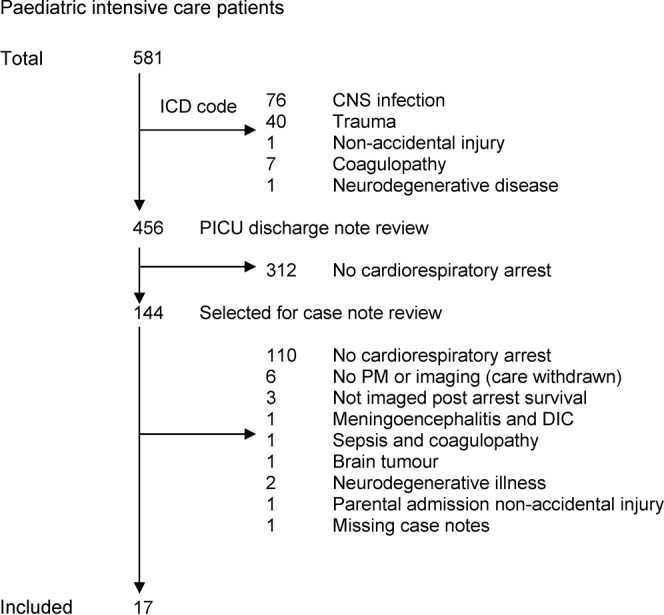
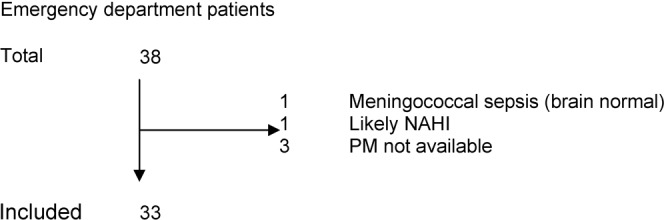
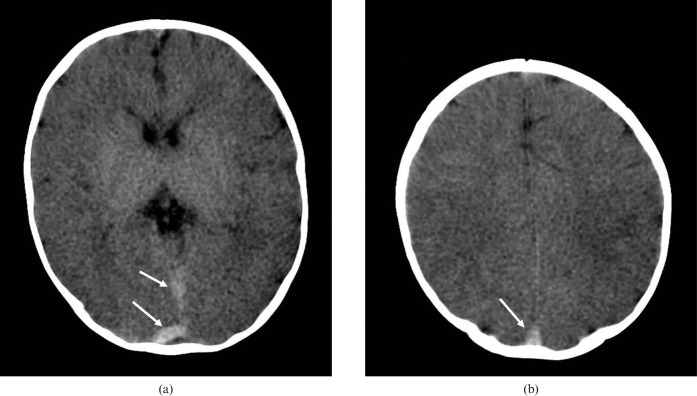
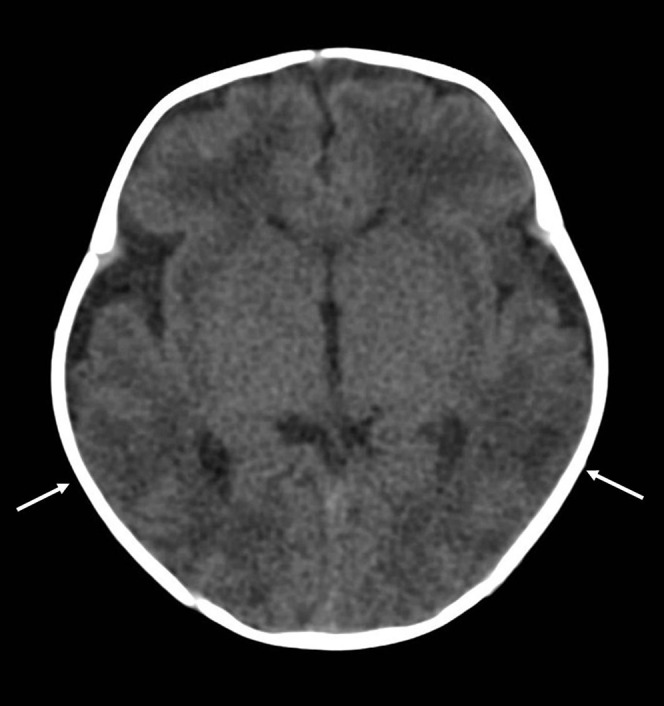
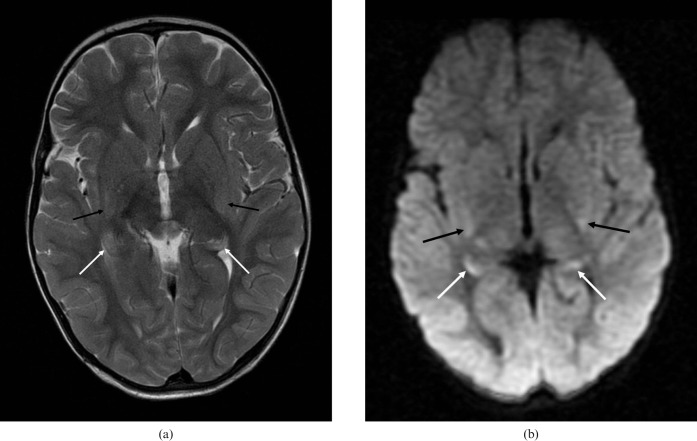
The aim of this study was to determine the frequency of subdural haematomas (SDHs) occurring in infants presenting following atraumatic cardiorespiratory collapse. This study was a review of retrospective case notes, brain imaging and post-mortem examinations carried out in the paediatric intensive care unit (PICU) and emergency department (ED) in a tertiary paediatric centre in the UK. The study included infants and children less than 4 years old dying in the ED or admitted to the PICU after atraumatic cardiorespiratory arrest. We identified macroscopic SDHs on brain imaging or post-mortem examination. Of those children who experienced a cardiorespiratory arrest from a non-traumatic cause and met inclusion criteria, 33 presented and died in the ED and 17 were admitted to the PICU. These children had a post-mortem examination, brain imaging or both. None of these infants had a significant SDH. One child had a small clot adherent to the dura found on post-mortem and two had microscopic intradural haemorrhage, but it is unclear in each case whether this was artefact, as each had otherwise normal brains. Subdural haematoma arising in infants or young children in the context of catastrophic cardiorespiratory compromise from a non-traumatic cause was not observed.
Figures
Similar articles
-
The neuropathology of infant subdural haemorrhage.Forensic Sci Int. 2009 May 30;187(1-3):6-13. doi: 10.1016/j.forsciint.2009.02.005. Epub 2009 Mar 19. Forensic Sci Int. 2009. PMID: 19303229 Review.
-
Subdural hemorrhage, intradural hemorrhage and hypoxia in the pediatric and perinatal post mortem: are they related? An observational study combining the use of post mortem pathology and magnetic resonance imaging.Forensic Sci Int. 2010 Jul 15;200(1-3):100-7. doi: 10.1016/j.forsciint.2010.03.036. Epub 2010 May 26. Forensic Sci Int. 2010. PMID: 20510556
-
Subdural haematomas and physical abuse in the first two years of life.Pediatr Neurosurg. 2007;43(5):352-7. doi: 10.1159/000106382. Pediatr Neurosurg. 2007. PMID: 17785998
-
Unexpected natural death of cerebral origin in medicolegal practice.Forensic Sci. 1975 Feb;5(1):11-9. doi: 10.1016/0300-9432(75)90082-5. Forensic Sci. 1975. PMID: 1132858
-
Investigating subdural haemorrhage in infants.Arch Dis Child. 2002 Feb;86(2):98-102. doi: 10.1136/adc.86.2.98. Arch Dis Child. 2002. PMID: 11827902 Free PMC article. Review.
Cited by
-
Consensus statement on abusive head trauma in infants and young children.Pediatr Radiol. 2018 Aug;48(8):1048-1065. doi: 10.1007/s00247-018-4149-1. Epub 2018 May 23. Pediatr Radiol. 2018. PMID: 29796797 Review.
-
Abusive head trauma: experience improves diagnosis.Neuroradiology. 2021 Mar;63(3):417-430. doi: 10.1007/s00234-020-02564-z. Epub 2020 Oct 20. Neuroradiology. 2021. PMID: 33079214 Free PMC article.
-
Prevalence and Risk Factors of Incidental Findings in Brain MRIs of Healthy Neonates-The FinnBrain Birth Cohort Study.Front Neurol. 2020 Jan 8;10:1347. doi: 10.3389/fneur.2019.01347. eCollection 2019. Front Neurol. 2020. PMID: 31969859 Free PMC article.
-
Alternate theories of causation in abusive head trauma: what the science tells us.Pediatr Radiol. 2014 Dec;44 Suppl 4:S543-7. doi: 10.1007/s00247-014-3106-x. Epub 2014 Dec 14. Pediatr Radiol. 2014. PMID: 25501725
References
-
- Mack J, Squier W, Eastman JT. Anatomy and development of the meninges: implications for subdural collections and CSF circulation. Pediatr Radiol 2009;39:200–10 - PubMed
-
- Cohen MC, Scheimberg I. Evidence of occurrence of intradural and subdural hemorrhage in the perinatal and neonatal period in the context of hypoxic ischemic encephalopathy. An observational study from two referral institutions in the United Kingdom. Pediatr Dev Pathol 2009;12:169–76 - PubMed
-
- Volpe JJ. In: Neurology of the newborn (5th edn).Hypoxic-ischemic encephalopathy: clinical aspects. Saunders,Philadelphia: Volpe JJ.2008;408–27
-
- Levene MI, de Vries LS. Levene MI, Chervenak FA.Fetal and neonatal neurology and neurosurgery. Neonatal incranial hemorrhage (4th edn).Philadelphia Churchill Livingstone,2009;395–430
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
