

CT and MRI in the evaluation of extraspinal sciatica
- PMID: 20647515
- PMCID: PMC3473399
- DOI: 10.1259/bjr/76002141
CT and MRI in the evaluation of extraspinal sciatica
Abstract
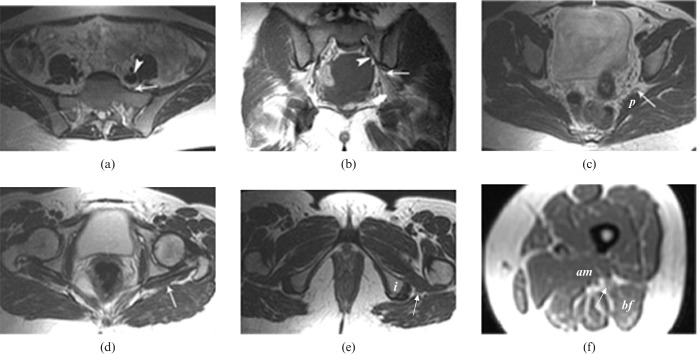
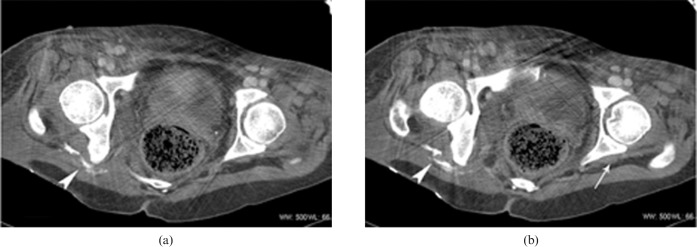
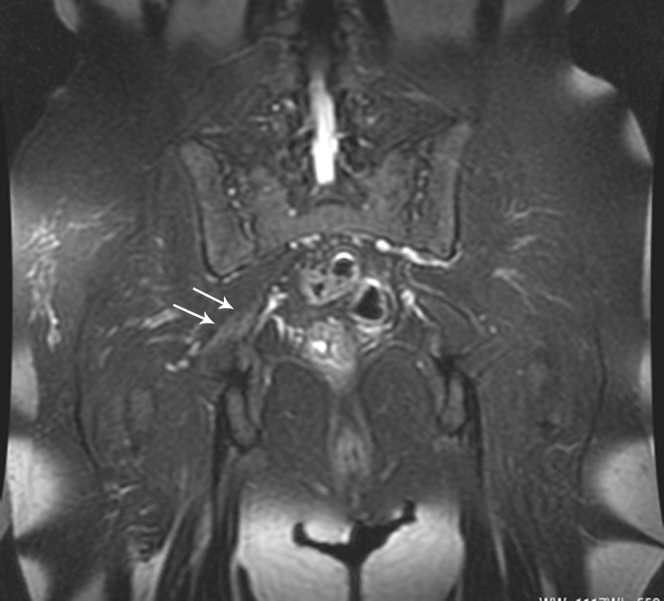
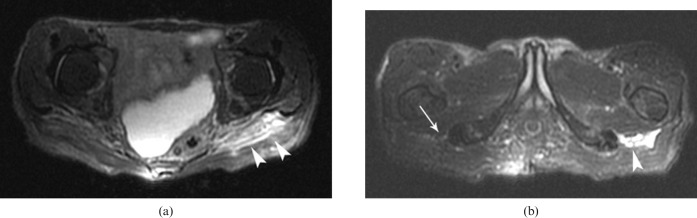
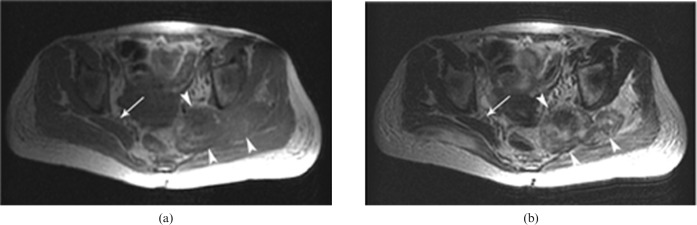
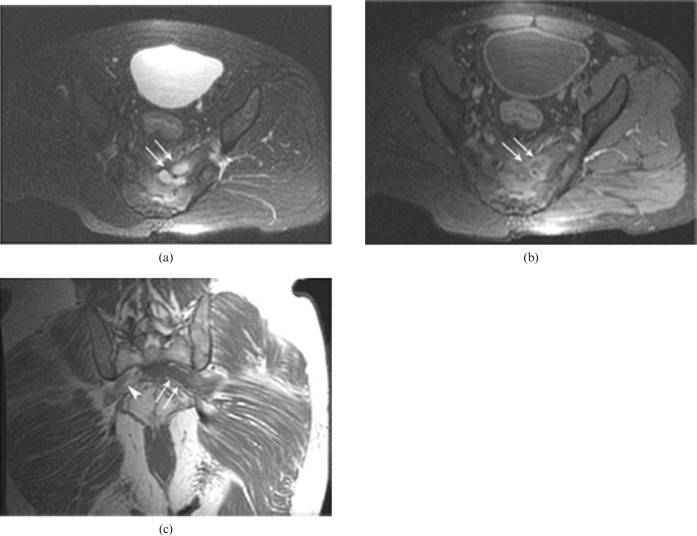
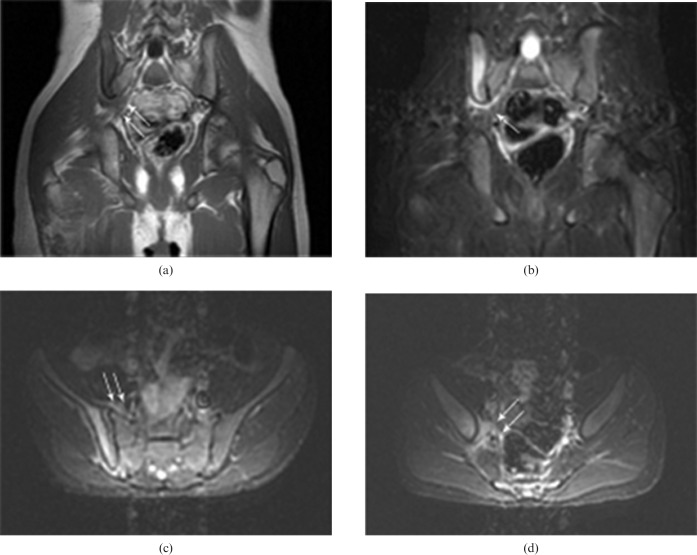
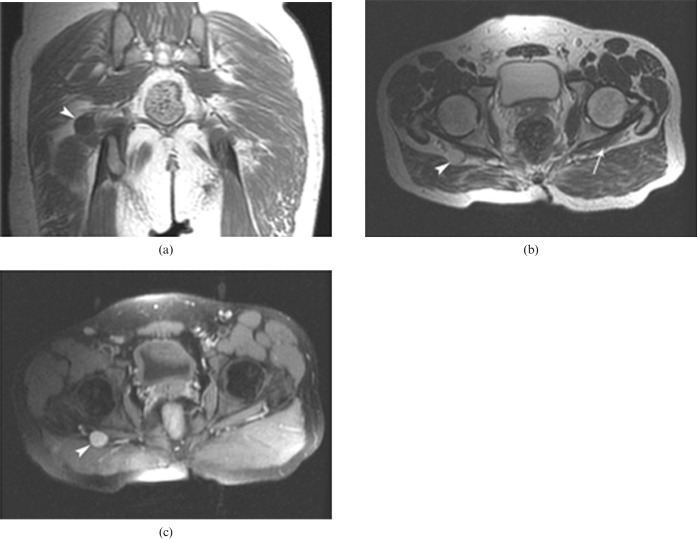
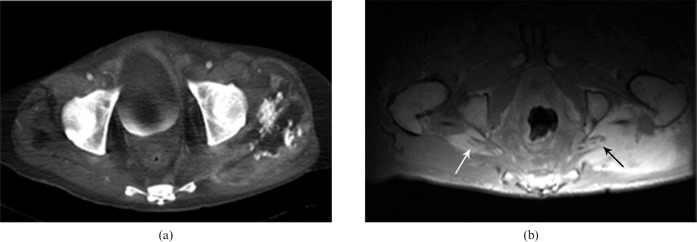
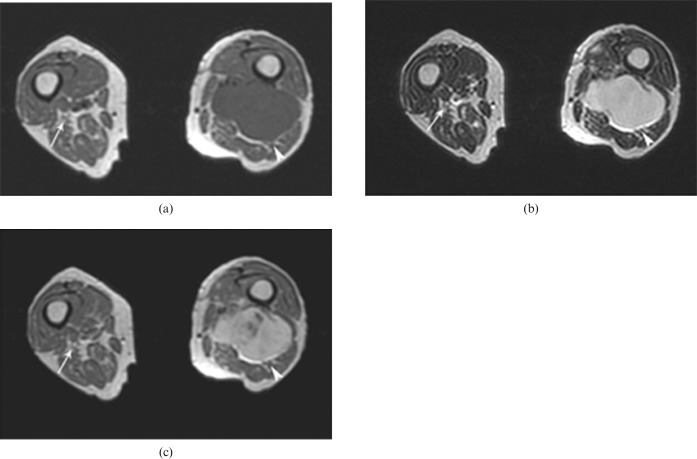
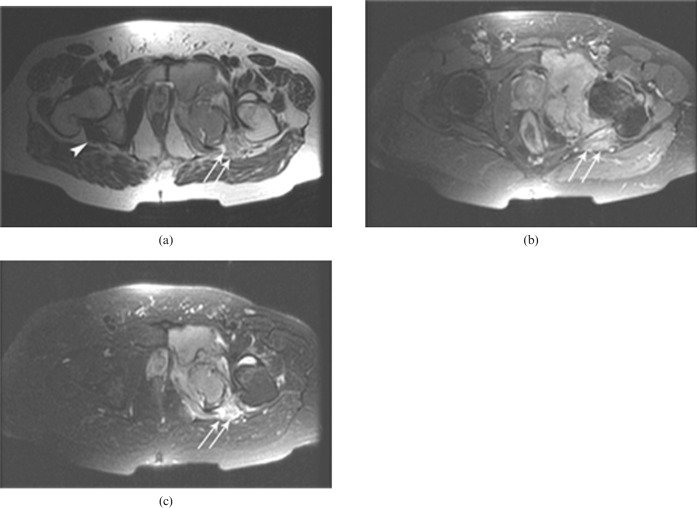
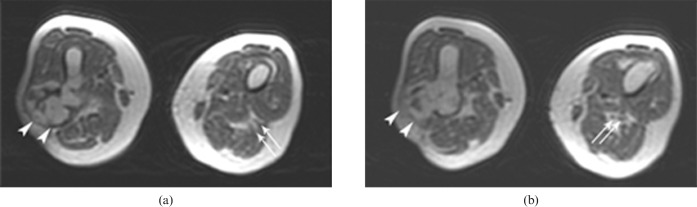
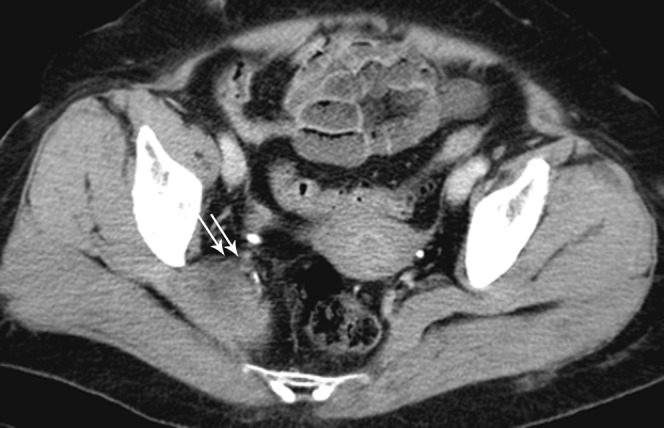
Sciatica is the most frequently encountered symptom in neurosurgical practice and is observed in 40% of adults at some point in their lives. It is described as pain of the hip and the lower extremity secondary to pathologies affecting the sciatic nerve within its intraspinal or extraspinal course. The most frequent cause is a herniating lumbar disc pressing on the neural roots. Extraspinal causes of sciatic pain are usually overlooked because they are extremely rare and due to intraspinal causes (lumbar spinal stenosis, facet joint osteoarthritis, fracture, and tumors of the spinal cord and spinal column) being the main consideration. Early diagnosis of sciatica significantly improves the likelihood of relieving symptoms, as well as avoiding any additional neurologic injury and unnecessary surgery. We evaluate histolopathologically confirmed extraspinal causes of sciatica cases, accompanied by their presented computed tomography and/or magnetic resonance imaging findings.
Figures



References
-
- Pick T, Howden R. Anatomy, descriptive and surgical (Gray's anatomy). Philadelphia, PA: Running Press, 1974: 781–93
-
- Moore KL, Dalley AF. Clinically oriented anatomy. Philadelphia, PA: Lippincott, Williams & Wilkins, 1999
-
- Villarejo FJ, Pascual AM. Injection injury of the sciatic nerve (370 cases). Childs Nerv Syst 1993;9:229–32 - PubMed
-
- Ergun T, Lakadamyali H, Derincek A, Cagla Tarhan N, Ozturk A. Magnetic resonance imaging in the visualization of benign tumors and tumor-like lesions of hand and wrist. Curr Probl Diagn Radiol 2010;39:1–16 - PubMed
