

Prevalence and risk factors for development of delirium in burn intensive care unit patients
- PMID: 20647937
- PMCID: PMC3773484
- DOI: 10.1097/BCR.0b013e3181eebee9
Prevalence and risk factors for development of delirium in burn intensive care unit patients
Abstract
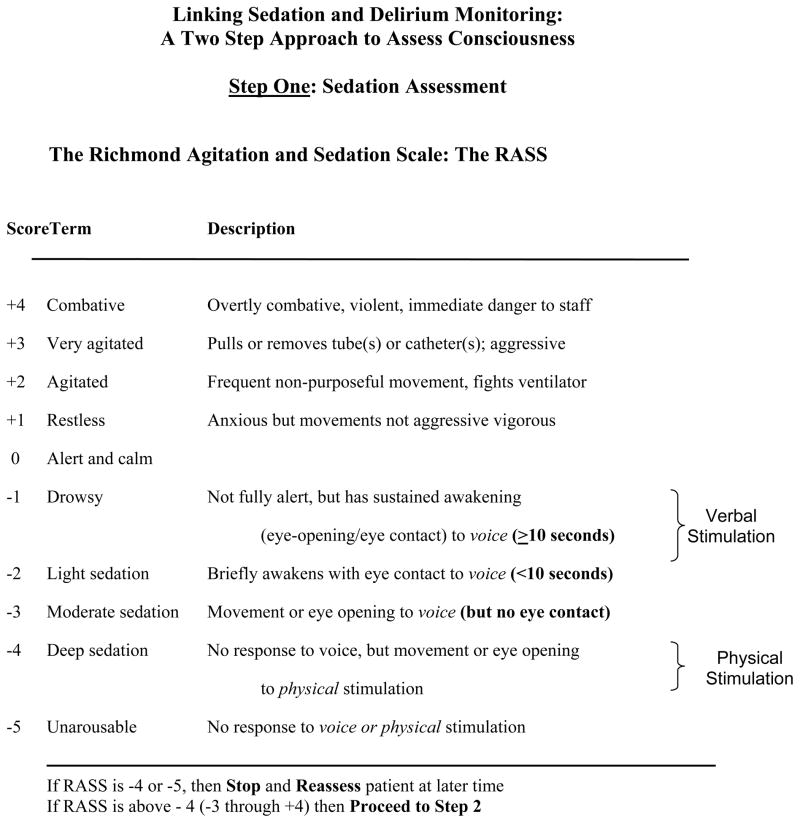
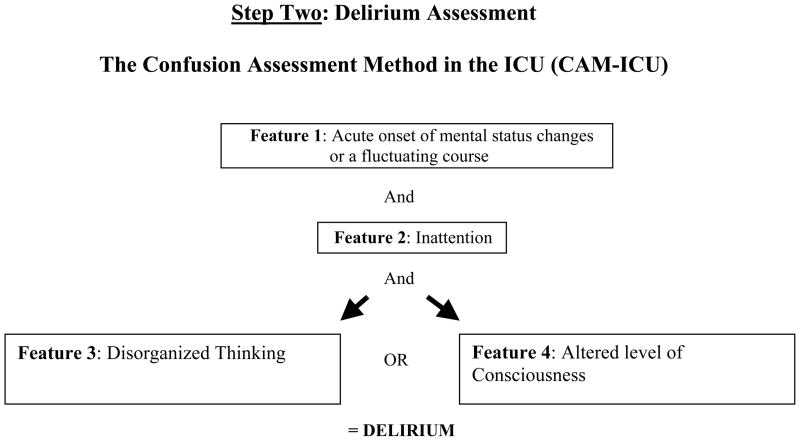
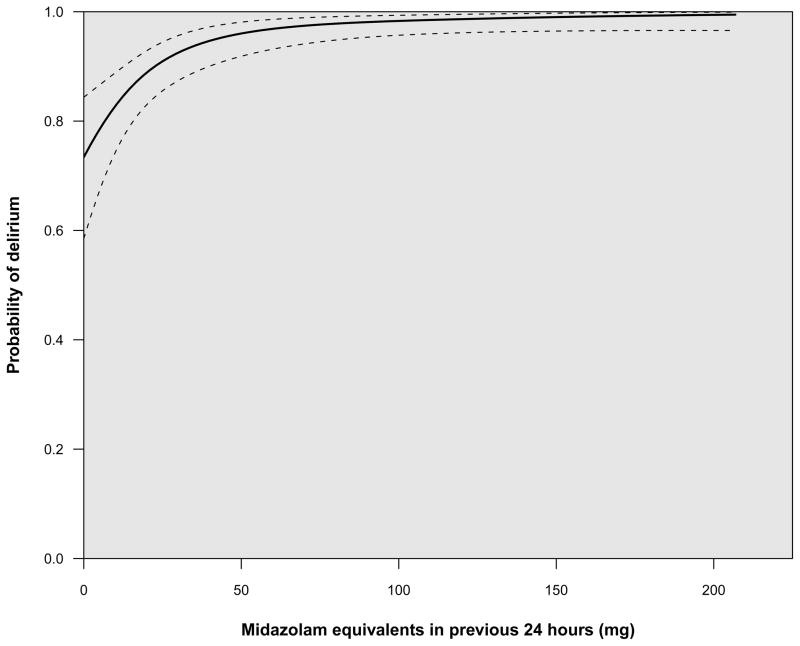
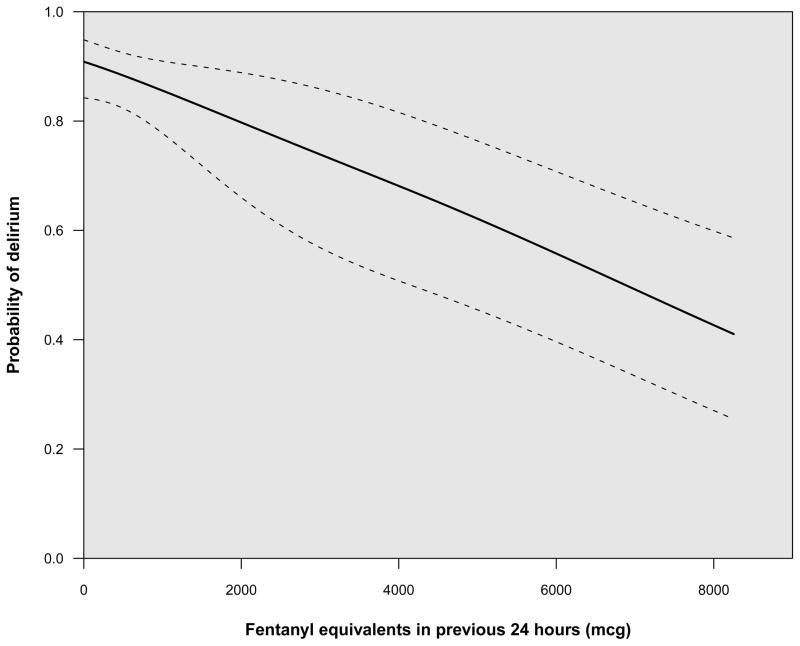
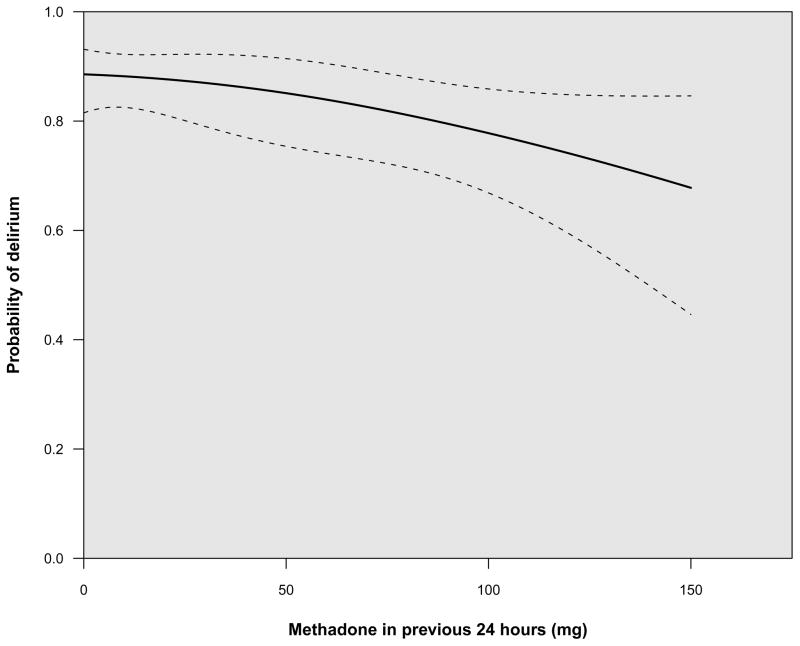
Delirium affects 60 to 80% of ventilated patients and is associated with worse clinical outcomes including death. Unfortunately, there are limited data regarding the prevalence and risk factors of delirium in critically ill burn patients. The objectives of this study were to evaluate the prevalence of delirium in ventilated burn patients, using validated instruments, and to identify its risk factors. Adult ventilated burn patients at two tertiary centers were prospectively evaluated for delirium using the Confusion Assessment Method in the Intensive Care Unit (CAM-ICU) for 30 days or until intensive care unit discharge. Patients with neurologic injuries, severe dementia, and those not expected to survive >24 hours were excluded. Markov logistic regression was used to identify the risk factors of delirium, adjusting for clinically relevant covariates. The 82 ventilated burn patients had a median (interquartile range) age of 48 (38-62) years, Acute Physiology and Chronic Health Evaluation II scores 27 (21-30), and percent burns of 20 (7-32). Prevalence of delirium was 77% with a median duration of 3 (1-6) days. Exposure to benzodiazepines was an independent risk factor for the development of delirium (odds ratio: 6.8 [confidence interval: 3.1-15], P < .001), whereas exposure to both intravenous opiates (0.5 [0.4-0.6], P < .001) and methadone (0.7 [0.5-0.9], P = .02) was associated with a lower risk of delirium. In conclusion, delirium occurred at least once in approximately 80% of ventilated burn patients. Exposure to benzodiazepines was an independent risk factor for delirium, whereas opiates and methadone reduced the risk of developing delirium, possibly through reduction of pain in these patients.
Conflict of interest statement
Dr. Pandharipande has received research grant and honoraria from Hospira Inc. Ms. Pun has received honoraria from Hospira Inc. Dr. Ely has received research grant and honoraria from Hospira, Inc, Pfizer, Eli Lilly, GSK, and a research grant from Aspect Medical Systems. The other authors report no financial disclosures.
Figures
References
-
- American Psychiatric Association. Diagnostic and statistical manual of mental disorders. 4. Washington, DC: American Psychiatric Association; 2000. text revision.
-
- Ely EW, Truman B, May L, et al. Validation of the CAM-ICU for delirium assessment in mechanically ventilated patients. J Am Geriatr Soc. 2001;49:S2.
-
- Ely EW, Inouye SK, Bernard GR, et al. Delirium in mechanically ventilated patients: validity and reliability of the confusion assessment method for the intensive care unit (CAM-ICU) JAMA. 2001;286:2703–2710. - PubMed
-
- Bergeron N, Dubois MJ, Dumont M, et al. Intensive Care Delirium Screening Checklist: evaluation of a new screening tool. Intensive Care Med. 2001;27:859–864. - PubMed
-
- Pun BT, Gordon SM, Peterson JF, et al. Large-scale implementation of sedation and delirium monitoring in the intensive care unit: A report from two medical centers. Crit Care Med. 2005;33:1199–1205. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
