

Contrasting predictors of poor antiretroviral therapy outcomes in two South African HIV programmes: a cohort study
- PMID: 20649946
- PMCID: PMC2920888
- DOI: 10.1186/1471-2458-10-430
Contrasting predictors of poor antiretroviral therapy outcomes in two South African HIV programmes: a cohort study
Abstract
Background: Many national antiretroviral therapy (ART) programmes encourage providers to identify and address baseline factors associated with poor treatment outcomes, including modifiable adherence-related behaviours, before initiating ART. However, evidence on such predictors is scarce, and providers judgement may often be inaccurate. To help address this evidence gap, this observational cohort study examined baseline factors potentially predictive of poor treatment outcomes in two ART programmes in South Africa, with a particular focus on determinants of adherence.
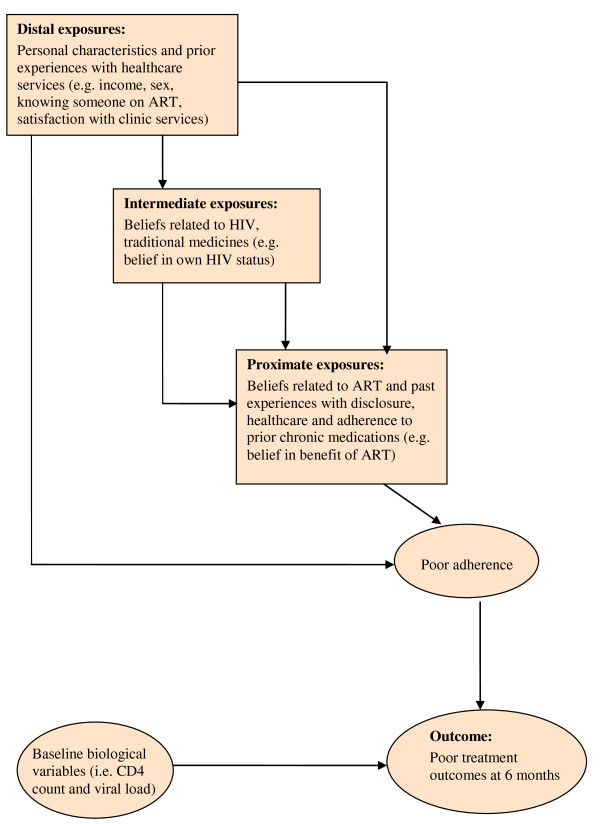
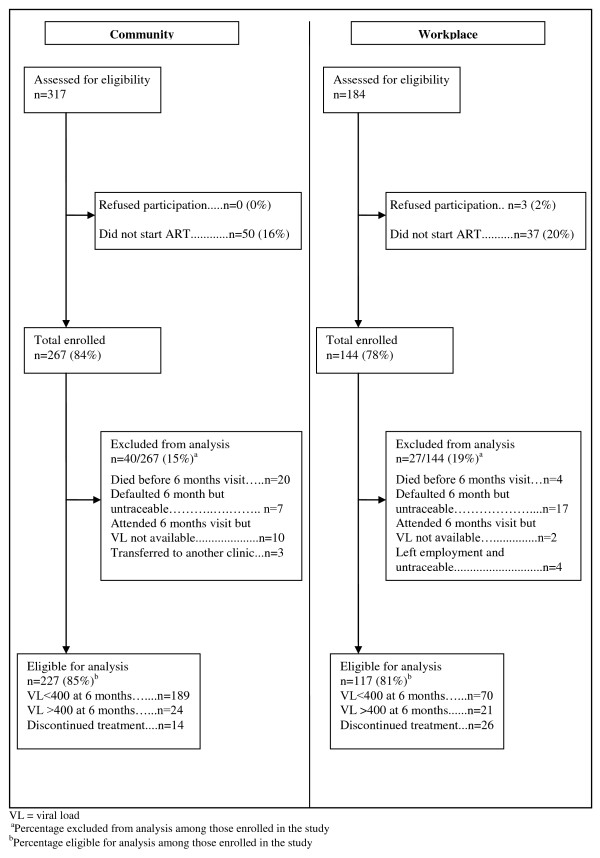
Methods: Treatment-naïve patients starting ART were enrolled from a community and a workplace ART programme. Potential baseline predictors associated with poor treatment outcomes (defined as viral load > 400 copies/ml or having discontinued treatment by six months) were assessed using logistic regression. Exposure variables were organised for regression analysis using a hierarchical framework.
Results: 38/227 (17%) of participants in the community had poor treatment outcomes compared to 47/117 (40%) in the workplace. In the community, predictors of worse outcomes included: drinking more than 20 units of alcohol per week, having no prior experience of chronic medications, and consulting a traditional healer in the past year (adjusted odds ratio [aOR] 15.36, 95% CI 3.22-73.27; aOR 2.30, 95%CI 1.00-5.30; aOR 2.27, 95% CI 1.00-5.19 respectively). Being male and knowing someone on ART were associated with better outcomes (aOR 0.25, 95%CI 0.09-0.74; aOR 0.44, 95%CI 0.19-1.01 respectively). In the workplace, predictors of poor treatment outcomes included being uncertain about the health effects of ART and a traditional healer's ability to treat HIV (aOR 7.53, 95%CI 2.02-27.98; aOR 4.40, 95%CI 1.41-13.75 respectively). Longer pre-ART waiting time (2-12 weeks compared to <2 weeks) predicted better treatment outcomes (aOR 0.13, 95% CI 0.03-0.56).
Conclusion: Baseline predictors of poor treatment outcomes were largely unique to each programme, likely reflecting different populations and pathways to HIV care. In the workplace, active promotion of HIV testing may have extended ART to individuals who, without provider initiation, would not have spontaneously sought care. As provider-initiated testing makes ART available to individuals less motivated to seek care, patients may need additional adherence support, especially addressing uncertainty about the health benefits of ART.
Figures
References
-
- The Joint United Nations Programme on HIV/AIDS. AIDS Epidemic Update. Geneva: UNAIDS; 2007. - PubMed
-
- World Health Organization, the Joint United Nations Programme on HIV/AIDS, United Nations Children's Fund. Towards Universal Access - Scaling up Priority HIV/AIDS Interventions in the Health Sector: Progress Report 2009. Geneva: WHO; 2009.
-
- Gifford AL, Bormann JE, Shively MJ, Wright BC, Richman DD, Bozzette SA. Predictors of self-reported adherence and plasma HIV concentrations in patients on multidrug antiretroviral regimens. J Acquir Immune Defic Syndr. 2000;10:386–395. - PubMed
-
- Haubrich RH, Little SJ, Currier JS, Forthal DN, Kemper CA, Beall GN, Johnson D, Dube MP, Hwang JY, McCutchan JA. The value of patient-reported adherence to antiretroviral therapy in predicting virologic and immunologic response. AIDS. 1999;10:1099–1107. doi: 10.1097/00002030-199906180-00014. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
