

HIV and risk environment for injecting drug users: the past, present, and future
- PMID: 20650523
- PMCID: PMC6464374
- DOI: 10.1016/S0140-6736(10)60743-X
HIV and risk environment for injecting drug users: the past, present, and future
Abstract
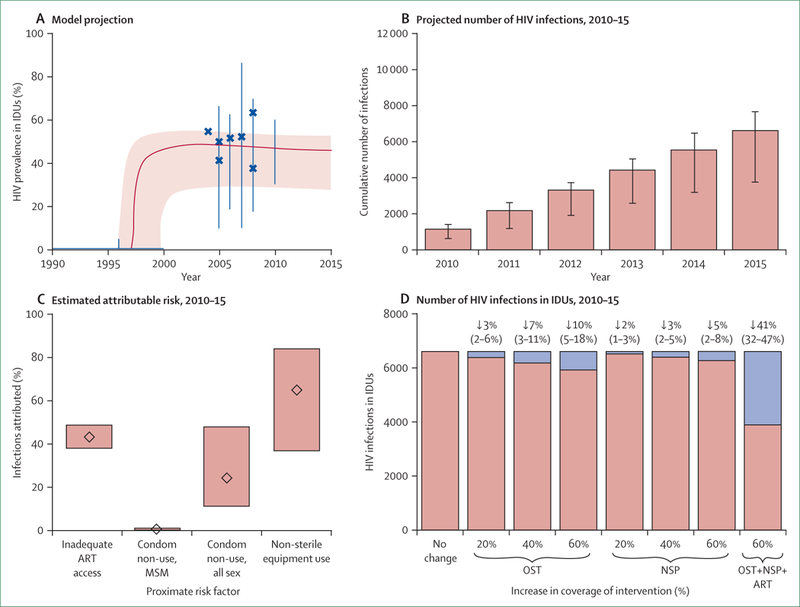
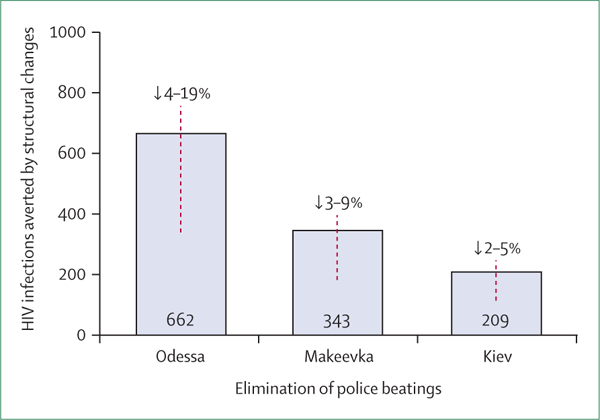
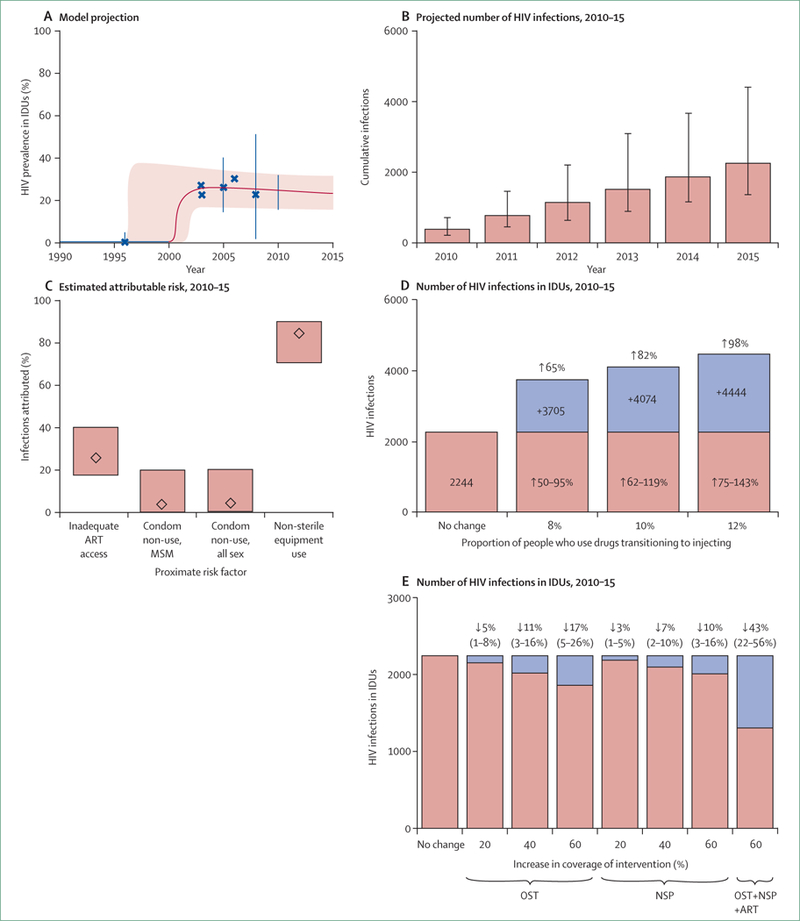
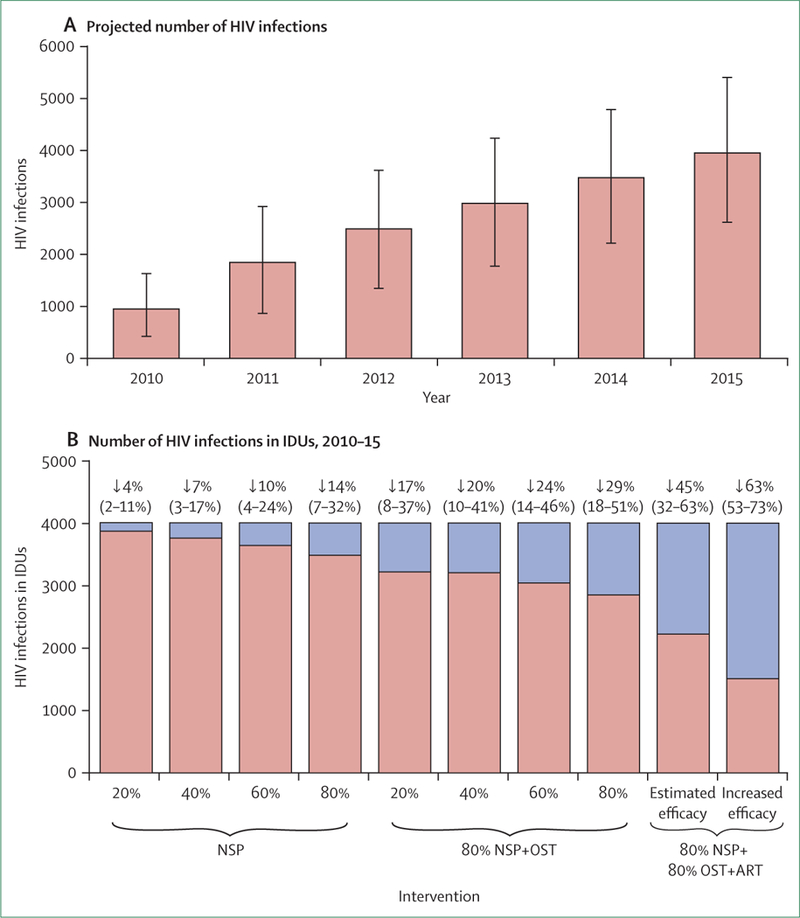
We systematically reviewed reports about determinants of HIV infection in injecting drug users from 2000 to 2009, classifying findings by type of environmental influence. We then modelled changes in risk environments in regions with severe HIV epidemics associated with injecting drug use. Of 94 studies identified, 25 intentionally examined risk environments. Modelling of HIV epidemics showed substantial heterogeneity in the number of HIV infections that are attributed to injecting drug use and unprotected sex. We estimate that, during 2010-15, HIV prevalence could be reduced by 41% in Odessa (Ukraine), 43% in Karachi (Pakistan), and 30% in Nairobi (Kenya) through a 60% reduction of the unmet need of programmes for opioid substitution, needle exchange, and antiretroviral therapy. Mitigation of patient transition to injecting drugs from non-injecting forms could avert a 98% increase in HIV infections in Karachi; whereas elimination of laws prohibiting opioid substitution with concomitant scale-up could prevent 14% of HIV infections in Nairobi. Optimisation of effectiveness and coverage of interventions is crucial for regions with rapidly growing epidemics. Delineation of environmental risk factors provides a crucial insight into HIV prevention. Evidence-informed, rights-based, combination interventions protecting IDUs' access to HIV prevention and treatment could substantially curtail HIV epidemics.
Copyright 2010 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Conflicts of interest
We declare that we have no conflicts of interest.
Figures
Comment in
-
Alcohol: the forgotten drug in HIV/AIDS.Lancet. 2010 Aug 7;376(9739):398-400. doi: 10.1016/S0140-6736(10)60884-7. Lancet. 2010. PMID: 20650516 Free PMC article. No abstract available.
References
-
- Mathers BM, Degenhardt L, Phillips B, et al. Global epidemiology of injecting drug use and HIV among people who inject drugs: a systematic review. Lancet 2008; 372: 1733–45. - PubMed
-
- Latkin CA, Forman V, Knowlton A, Sherman S. Norms, social networks, and HIV-related risk behaviors among urban disadvantaged drug users. Soc Sci Med 2003; 56: 465–76. - PubMed
-
- Des Jarlais DC, Arasteh K, Perlis T, et al. Convergence of HIV seroprevalence among injecting and non-injecting drug users in New York City. AIDS 2007; 21: 231–35. - PubMed
-
- Booth RE, Kwiatkowski CF, Brewster JT, Sinitsyna L, Dvoryak S. Predictors of HIV sero-status among drug injectors at three Ukraine sites. AIDS 2006; 20: 2217–23. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
